|
Thomas Zgonis, DPM, FACFAS - Associate Professor, Department of Orthopaedic Surgery
- Chief, Division of Podiatric Medicine and Surgery
- Director, Podiatric Surgical Residency and Reconstructive Foot and
- Ankle Fellowship
- The University of Texas Health Science Center at San Antonio
- San Antonio, Texas
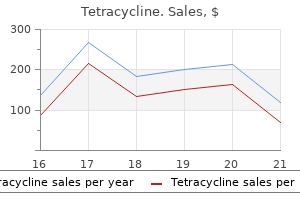
Tetracycline dosages: 500 mg, 250 mg
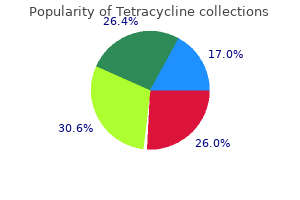
Tetracycline packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Purchase 500 mg tetracycline visaThe current function of the synthetic urinary sphincter for the remedy of urinary incontinence virus going around purchase tetracycline line. The male bulbourethral sling procedure for post-radical prostatectomy incontinence. Urethral compression for the remedy of postprostatectomy urinary incontinence: Is historical past repeating itself Transobturator sling suspension for male urinary incontinence together with post-radical prostatectomy. Urodynamic analysis of a suspension method for fast recovery of continence after radical retropubic prostatectomy. Early results of transobturator sling suspension for male urinary incontinence following radical prostatectomy. Can advance transobturator sling suspension cure male urinary postoperative stress incontinence Surgery insight: surgical administration of postprostatectomy incontinence�the synthetic urinary sphincter and male sling. Intermediateterm outcomes, as much as four years, of a bone-anchored male perineal sling for treating male stress urinary incontinence after prostate surgery. Bone anchor infections in female pelvic reconstructive procedures: a literature evaluate of series and case stories. Longterm efficacy of the bone-anchored male sling for moderate and extreme stress urinary incontinence. Menstrual age or gestational age of pregnancy is the duration of pregnancy calculated from the primary day of the last menstrual interval. Gestational age is often taken to be equal to 10 lunar months or 9 calendar months and seven days or 280 days or 40 weeks. Thus, true gestational age is the identical as 280 days minus 14 days, which is equal to 266 days. The entire period of pregnancy may be divided in to three phases: the first trimester: 1�12 weeks; second trimester: 3�27 weeks and the third trimester: 28�40 weeks. However, if the pregnancy does happen, the perform of corpus luteum must be maintained so as to guarantee sustained progesterone manufacturing. Between 6� eight weeks of gestation, the features of corpus luteum get transferred to placenta and it turns into answerable for manufacturing of protein and steroid hormones, that are liable for various bodily and physiological changes. This hormone could be detected in maternal plasma or urine by 8�9 days following ovulation. It antagonizes the action of insulin and causes lipolysis, proteolysis and promotes the switch of glucose and amino acids to the fetus. For steroidogenesis, it relies upon upon the precursors derived from the fetal and partly from the maternal sources. Second Trimester of Pregnancy There is disappearance of subjective symptoms of being pregnant similar to nausea, vomiting and frequency of micturition. Other symptoms, which may appear include the followings: Abdominal enlargement: Progressive enlargement of the lower stomach happens as a end result of the growing uterus Fetal actions: Fetal movements typically happen after 18�20th week of gestation Quickening: Fetal movement (quickening) can usually be seen or heard between 16�18 weeks of gestation in a multigravida. A primigravida, however, is able to appreciating fetal actions after roughly 2 weeks. Lightening is another phenomenon, which happens at approximately 38 weeks of gestation particularly in the primigravida. This ends in a slight reduction in fundal peak, which offers aid in opposition to pressure signs Frequency of micturition: There is an increased frequency of micturition, which had beforehand disappeared in the second trimester Fetal actions turn into more pronounced: the fetal movements become more pronounced and palpation of fetal elements becomes easier Braxton Hicks contractions turn out to be more evident Fetal lie, presentation and period of gestation could be decided. In this test, a monoclonal antibody against subunit is bound to a solid-phase assist. In some assays, the second antibody is linked to an enzyme such as alkaline phosphatase. When the substrate for the enzyme is added, a color develops, depth of which is proportional to the quantity of enzyme and, subsequently, to the amount of second antibody sure. By 35 days of gestation, a standard sac is visible in all ladies and by 6 weeks, fetal cardiac activity can be visualized. Up to 12 weeks, the crown-rump size is predictive of gestational age inside 4 days. Similarly, a yolk sac bigger than 7 mm with out evidence of a creating fetal pole suggests a nonviable pregnancy. Low progesterone ranges are observed in instances of ectopic pregnancy and abortion, whereas high progesterone values are observed in cases of hydatidiform mole, Rh isoimmunization, and so forth. The testes are liable for producing sperms and male hormone, primarily testosterone. Testosterone is synthesized in the interstitial leydig cells from where it diffuses in to the seminiferous tubules and plays an necessary function in the facilitation of the process of spermatogenesis, which involves the production of sperms. Initial process of spermatogenesis includes mitotic division, which is answerable for changing spermatogonia to major spermatocytes. The spermatozoa then develop through a means of meiosis so that ultimately diploid spermatocytes get converted in to four haploid spermatids. The primordial germ cells, after arriving within the female gonad, differentiate in to oogonia around 9th week of gestation. Progression of meiosis to the diplotene stage is accomplished throughout the pregnancy and is accomplished by start. Second meiotic division starts, however will get arrested in the metaphase, which is completed only at the time of fertilization. Once the oocyte has been extruded out, the cells of the empty ovarian follicle get converted in to the corpus luteum which produces progesterone for about 14 days, in absence of fertilization and for 3�4 months if fertilization has taken place, after which it will definitely dies off. The oocyte moves from the ovary to the uterine tube and will get fertilized by the male gamete within the ampulla of the uterine tube. Even although many spermatozoa could approach the oocyte, only one spermatozoon is allowed to enter the oocyte. The means of fertilization between two haploid gametes ends in the formation of a diploid zygote, thereby restoring the number of chromosomes to that of the traditional somatic cell. Cleavage Division and Formation of Morula the zygote, a diploid cell with 46 chromosomes, fashioned because of fertilization of mature egg with a sperm undergoes numerous cleavage divisions to produce cells generally identified as blastomeres. At this stage the zygote is present contained in the fallopian tube and is surrounded by a thick zona pellucida. The morula enters the uterine cavity roughly 3 days after fertilization, and floats around in the cavity for a couple of more days. Formation of Blastocyst When the blastocyst reaches 58-celled stage at about 4�5th day of fertilization, it will get reworked in to two forms of cells: (1) trophoblast cells and (2) an inside cell mass. The internal cell mass (consisting of blastomeres) is destined to form the various tissues of the embryo. Implantation begins with the burrowing of the blastocyst in to the endometrium, which happens by about 6�7 days after fertilization. By 8 day postfertilization, the trophoblast gets differentiated in to an outer multinucleated syncytium known as syncytiotrophoblast and an inner layer of cytotrophoblasts. As the trophoblastic cells invade deeper in to the endometrium, by tenth day postfertilisation the blastocyst gets totally embedded within the endometrium. As the blastocyst implants in to the uterine wall, concurrently it also prepares its cells and surrounding endometrium to develop in to a placenta.
Cheap tetracycline 250mg visaThis is done not with the intent to eradicate colonization antibiotic for sinus infection and sore throat buy cheap tetracycline 500 mg on line, but somewhat to prevent septicemia in the course of the manipulation. Many cases are managed with acute dilation, but this is in all probability not in the best curiosity of the affected person. A suprapubic cystostomy catheter can be used to deal with the acute retention and give time to plan extra applicable treatment. The anatomy of the stricture must be determined both through advanced imaging or versatile endoscopy, which at least, allows the stricture to be visualized and a guidewire to be passed beneath direct vision through the lumen. In addition to etiology, the situation, size, depth, and density of the stricture (spongiofibrosis) or stenosis have to be accurately decided so as to develop a workable treatment plan. The length and placement of the stricture may be decided with conventional radiography, urethroscopy, and/or ultrasonography. Some really feel that absolutely the length of spongiofibrosis is most likely not evident by ultrasound analysis alone. Contrastenhanced research could also be further complemented by the addition of ultrasound research and together these are accurate in figuring out the length of narrow-caliber annularity [7]. Contrast studies of the urethra are best carried out by or beneath the direct supervision of the surgeon answerable for remedy of the affected person. The depth and density of the scar in the spongy tissue are difficult to determine, but are subjectively greatest evaluated by physical examination, contrast-enhanced studies that show the appearance of the urethra, and elasticity and appearance of the mucosa by endoscopy. Bladder neck stenosis usually responds nicely to endoscopic management, by mild dilation or incision utilizing cold knife, electrocautery or laser methods. A more extreme form of bladder neck stenosis termed vesicourethral distraction stenosis could be a devastating consequence of radical prostatectomy. Posterior urethral distraction defects are commonly seen with anterior pelvic arch fractures. It has been classically taught that these fractures trigger the prostatic apex to separate from the membranous urethra within the method during which an apple is removed from its stalk. Newer knowledge, however, show that these injuries sometimes occur extra distally than the extent of the prostatic apex [5, 6]. The stage of the distraction defect is usually found simply proximal to the departure of the bulbous urethra from the membranous urethra, and thus spares the exterior urinary sphincter. As in a vesicourethral distraction, this damage results in extensive fibrosis interposed between the 2 distracted ends of the urethra and is immune to endoscopic management. Compensatory hypertrophy of the detrusor could initially allow patients to void by way of a narrowed urethral lumen with few symptoms. Additionally, some degree of decreased urethral caliber might not considerably affect the circulate dynamics. Patients might not develop vital symptoms until a reduced urethral caliber of 10�12F is reached. Many of those patients will relate an insidious onset of voiding symptoms before progressing to obstructive signs or full obstruction. First, you will need to question the affected person as to the historical past of trauma, particularly straddle trauma. A historical past of urethral infection, earlier urethral, prostate or bladder surgical procedures, and previous catheterizations must be famous. Stigmata of hypospadias, lichen sclerosis, previous surgical interventions, and spongiofibrosis could additionally be discovered. These clues revealed by historical past and bodily examination might give the practitioner extra data as to the etiology of the illness Chapter 139 Incision: Endoscopic Management of Urethral Stenoses spongiofibrosis and site of the defect, we find these research to rarely affect the remedy plan developed with traditional radiography and endoscopy. At our heart, imaging contains retrograde urethrography as properly as voiding cystourethrography. The affected person is positioned in a steep lateral oblique place as anteroposterior pictures typically can miss lesions or misrepresent their length. It must also be understood that in contrast-enhanced urethrography, multiple projection may be necessary to visualize the stricture. Realtime ultrasound analysis of the urethra after it has been filled with a lubricating jelly or saline has been described by Morey and McAninch [7, 8]. It is a misconception, however, that ultrasonography at all times immediately visualizes the spongiofibrosis. Morey 1655 and McAninch, nonetheless, believe that ultrasonography of the bulbous urethra presumably extra accurately determines the size of the stricture, which is essential in contemplating an anastomotic repair [7, 8]. An preliminary endoscopic examination with the versatile cystoscope may be necessary after the distinction studies to consider the urothelium and assess the degree of spongiofibrosis. A pediatric cytoscope is a really useful tool to help traverse an space of narrow-caliber illness with out having to dilate it, as dilation will not be finally beneficial. Care must be taken to avoid inciting irritation of a particularly narrow stricture by passage of the pediatric endoscope. This analysis allows delineation of the proximal point of the stricture by endoscopy, and the distal point by retrograde urethrography carried out concurrently. We imagine the safest method presently out there is the use of urethral balloon dilation. These catheters could also be hooked up to a filiform tip or handed over a guidewire with an integral Coud� tip. A residence balloon obturation protocol can then be carried out by the affected person with the objective of maintaining the operative dilation. This minimizes the amount of repetitive trauma to the urethra and permits the therapeutic process to stabilize, while being periodically opposed by the house balloon protocol. We choose to have the patient use a steroid cream as lubricant for the balloon to lower urethral inflammation. Initially, the patient begins the obturations a quantity of times every day, then day by day, then weekly, after which steadily decreasing the frequency as the method permits. This protocol allows for remedy of most types of urethral stricture/ stenosis, although as previously stated, distraction defects of the posterior urethra are very difficult to manage in this trend. Meatal dilation in circumstances of meatal stenosis secondary to lichen sclerosis has additionally been proven to be an effective administration strategy. It is type of straightforward for sufferers to carry out home dilations utilizing a graduated dilator lubricated with steroid cream. The affected person have to be completely recommended on correct technique and the objectives of dilation if this is to achieve success. Frequent, nonaggressive episodes of dilation are favored over periodic forceful episodes. In addition to limiting trauma, the patient will normally discover this to be extra snug, as little or no ache and no bleeding ought to be encountered. By limiting the quantity of distal obstruction, proximal dilation and extravasation also wants to be minimized, thus decreasing proximal irritation and probably stricture formation. With initial persistence and patience, many patients discover that eventually the meatal process stabilizes and only infrequent interventions are needed. Compensatory detrusor hypertrophy in cases of longstanding outlet obstruction could result in myogenic detrusor failure.
Order discount tetracyclineWhile bicarbonate and mannitol have been used in makes an attempt at renal protection virus back pain cheap 250mg tetracycline mastercard, hydration alone has proven enough within the therapy of myoglobinuria that accompanies the deep muscle necrosis and acidosis in these accidents. These embody loss of consciousness (75%), amnesia, paresthesias (80%) and keraunoparalysis. These embody hypoxic ischemic neuropathies, intracranial hemorrhage, post-arrest cerebral infarctions and cerebellar syndromes. Group 3 neurologic effects are probably delayed syndromes, including motor neuron diseases and motion disorders. Finally, group 4 injuries similar to subdural or epidural hematomas occur because of associated falls or blasts. Myoglobinuria the most typical causes of dying from lighting damage are cardiopulmonary arrest and apnea. The interruption of normal cardiac conduction by the associated direct current results in asystole, but like a defibrillator, spontaneous cardiac exercise sometimes resumes shortly thereafter. Answer: B Blumenthal R (2005) Lightning fatalities on the South African Highveld: a retrospective descriptive study for the interval 1997 to 2000. Early burn wound excision and grafting, of deep second- and third-degree burns is associated with: A. The persistence of those burned tissues function a nidus for irritation and an infection that can lead to sepsis and dying. Early excision and grafting of these wounds is now practiced in most burn facilities, and has been associated with improved survival, decreased blood loss and shorter hospitalizations. All of the above are just as prone to minimize threat Mafenide acetate is the greatest choice for this location, as it has the most effective eschar or cartilaginous penetration. Involvement of the testicle suggests an intraabdominal or retroperitoneal source of infection E. Etiology could be discovered within the majority of cases, and contains urogenital causes (urethral strictures), anorectal processes (abscesses, malignancies), trauma (bites, stings, blunt trauma), cutaneous processes (cellulitis), and retroperitoneal occasions (psoas and perinephric abscesses, appendicitis, pancreatitis). Consequently, retroperitoneal infections can unfold along the inner and external fascial layers of the spermatic cord. The testis, bladder, and rectum are hardly ever involved, as a end result of the fact that their blood supply derives from the aorta. Testicular involvement particularly suggests an intraabdominal or retroperitoneal supply on an infection. It incessantly presents with sudden onset of severe unilateral ache accompanied by nausea and vomiting B. History of intermittent ache somewhat than acute onset of unrelenting pain guidelines out torsion E. Radionuclide scanning and scrotal ultrasound can affirm the analysis Testicular torsion is the only explanation for the acute scrotum that mandates emergent diagnosis and remedy. Patients typically current with acute onset of unilateral ache, accompanied by nausea and vomiting. Paraphimosis, or entrapment of a retracted foreskin behind the coronal sulcus, is a surgical emergency, and requires instant discount so as to keep away from the attainable sequellae of ischemia of the foreskin and glans. Common causes of paraphimosis embody failure to replace the foreskin after Foley catheterization or voiding/bathing, vigorous sexual activity, or continual balanoposthitis. The ordinary first intervention is guide discount, which may be facilitated by software of ice. The osmotic methodology involves wrapping the penis in gauze, and making use of a hypertonic answer such as 3% saline or 50% dextrose. The puncture methodology involves using a 21�26 gauge needle to make circumferential punctures in the edematous foreskin, releasing the trapped liquid. Injection of hyaluronidase in 1 mL doses in to the foreskin is an alternative choice; the hyaluronidase is felt to scale back the edema by breaking down the hyaluronic acid in the extracellular fluid. Aspiration of 3�12 mL of blood from the corpora (after initiation of a penile block and placement of a tourniquet) may permit for discount of the paraphimosis. As properly, a history of intermittent pain is in preserving with the analysis, in that serial torsion and spontaneous detorsion could also be occurring. The involved testicle may be excessive driving, or lie transversely rather than vertically. The length of tolerance of the ischemic insult is dependent upon the diploma of twisting, however usually torsion should be relieved within four to eight hours. Imaging options embody high resolution scrotal ultrasound with color Doppler and radionuclide scanning. The contralateral testis is then examined and orchidopexy carried out with three absorbable sutures. The detorsed testis is then re-examined, and decision made relating to orchidopexy versus orchiectomy. Which of the next is incorrect regarding the analysis and administration of a man who presents with priapism Total parenteral nutrition may cause the ischemic type Priapism is outlined as persistence of erection beyond 4 hours, in the absence of sexual stimulation. It is important to distinguish between the 2 because of the distinction in administration. In ischemic priapism, occlusion of venous outflow results in cessation of arterial influx, creating an acidotic and hypoxic milieu throughout the corpora, which will lead to fibrosis, necrosis, and erectile dysfunction. Injection of sympathomimetic brokers, ideally phenylephrine, is the following step within the algorithm. Either a biopsy needle or a scalpel is used to create a fistula between the corpus cavernosum and the glans/corpus spongiosum/veins. Non-ischemic, or "high-flow" priapism, then again, is a nonemergent situation. Trauma to the penis, perineum, or pelvis, causes rupture of an artery, typically a branch of the cavernosal artery, leading to increased arterial inflow to the penis. Appropriate historical past, physical (perineal bruising and a semi-erect, nonpainful penis), and ultrasound, which demonstrates ruptured cavernosal artery with unregulated blood move, diagnose this situation. Use of ice packs along side expectant management is an inexpensive first strategy, and could also be profitable in up to 62% of cases. A C5 quadriplegic affected person is dropped at the emergency department three weeks after discharge from the trauma service. The patient stories a sense of tension, in addition to onset of headaches accompanied by nausea. Physical examination reveals a barely anxious patient lying in supine position, with attainable gentle distention of the decrease stomach. Which preliminary intervention is most likely to remove the trigger for this dysfunction The syndrome is often seen in patients with damage at or above T6, and is extra frequent with cervical rather than thoracic backbone accidents. Stimuli including bladder distention, urinary tract an infection, bowel distention, fecal impaction, perianal processes, ingrown toenails, pressure sores, and fractures ship a stimulus to the spinal wire via peripheral nerves.
Order 500mg tetracycline with amexMay produce speaking hydrocephalus as a complication Subarachnoid hemorrhage is likely considered one of the most typical intracranial hemorrhages following head harm antibiotics jaw pain buy tetracycline cheap. Rarely subarachnoid hemorrhage leads to progressive communicating hydrocephalus that requires shunting. Which of the statements concerning subarachnoid hemorrhage following trauma is right Zone of injury is the first determinant of operative versus non-operative administration E. Soft signs of vascular harm embrace non-expanding and non-pulsatile hematomas or minor bleeding from the injury. Soft signs of aerodigestive damage include odynophagia, small hemoptysis or hematemasis, hoarseness, or minor subcutaneous emphysema. Currently the primary determinant of operative versus conservative administration is clinical presentation. Patients with hard signs of vascular or aerodigestive injury require surgical exploration no matter location of harm, these with soft signs bear imaging. Hard signs of vascular injury include arterial bleeding, pulsatile or increasing hematoma, lack of pulse distal to the harm, bruit or thrill on the harm web site, unexplained shock or anemia. Hard signs of aerodigestive damage embrace bubbling from the harm website, large quantity hemoptysis or hematemasis, stridor, or large Surgical Critical Care and Emergency Surgery: Clinical Questions and Answers, First Edition. Because the patient is secure one of the best course of action is to proceed instantly to the operating room for definitive airway control with fiberoptic intubation followed by surgical exploration. Direct laryngscopy will not be tolerated well in the awake patient, and drugs utilized in speedy sequence intubation may convert an urgent airway in to an emergent airway. Direct laryngoscopy may also be technically difficult due to distortion of the airway from the hematoma. Cricothyroidotomy is an efficient possibility for the unstable patient, but should only be used if endotracheal intubation fails within the stable affected person. In a affected person with cervical spinal twine injury, which pulmonary perform check best predicts deteriorating lung operate Residual volume is elevated and no change is noted in useful residual capacity. Respiratory issues happen in 36�83% of patients, and a big proportion will require mechanical ventilation. Injury above C5 will end in lack of phrenic nerve function; under C5 loss of accessory muscles inhibit pulmonary operate. Because these sufferers are challenging airways, many advocate early elective intubation. Strong consideration must be given to serial evaluation of vital capacity in these sufferers as decreased important capacity may precede medical proof of respiratory compromise. Vital capability below 10 mL/kg of ideal physique weight is a sign for urgent intubation. It is the identical as the inspiratory reserve quantity plus the tidal volume plus the expiratory reserve quantity. Answer: C Berlly M and Shem K (2007) Respiratory administration during the first five days after spinal wire damage. Upon exploration, a laceration to the anterior trachea is famous throughout the primary and second tracheal rings. Exposure of the brachiocephalic vein Neck exploration for trauma is performed via a longitudinal incision along the anterior border of the sternocleidomastoid. The presence of an anterior tracheal damage makes evaluation of the posterior wall of the trachea and the esophagus of paramount importance, as concomitant injuries are present in 10-15% of instances. It also avoids the morbidity associated with an arterial puncture and uses a lower contrast dose than traditional angiography. Studies have shown detection charges much like historic controls with 4 vessel angiography. Injuries can happen on account of severe hyperextension or rotation, direct drive to the vessel, or by harm from adjoining fractures. The presence of a seat belt signal on the neck is controversial as a sign for screening, and in the absence of other danger components is unlikely to indicate damage. However, with fashionable imaging, if the fracture line of the basilar skull fracture is clear and not involving the carotid or vertebral openings, there will be lower yield within the screening course of and might be not indicated. The majority of low grade injuries heal, and repeat imaging is indicated as antithrombotic remedy can be discontinued after healing. Surgery could be thought of for accessible lesions, and endovascular treatment for inaccessible lesions. Grade V lesions (active extravasation) require surgical procedure or endovascular intervention. This uncommon complication can be averted by strict use of the oral route for gastric decompression in sufferers with proof of facial or basilar skull fractures. The complication seen beneath may be prevented in patients with craniofacial trauma by which of the following Inability to obtain an erection Lateral skull radiograph demonstrating an intracranial nasogastric tube E. Infertility in males the reproductive system of each men and women can be affected by spinal cord damage. Women may undergo a short lived interruption of menses, which typically resolves inside 6�9 months of injury. They might undergo from low testosterone, and, while erection is feasible, ejaculation is unlikely in the absence of vibrational or electrical stimulation gadgets. Skowronski E, Hartman K (2008) Obstetric management following traumatic tetraplegia: Case sequence and literature evaluation. All esophageal repairs ought to be buttressed with healthy tissue; that is of paramount significance if other suture strains are current. Buttressing could be carried out with one of many strap muscular tissues, or the sternocleidomastoid. Drains will help stop hematoma formation, which may lead to acute airway obstruction, and can management potential esophageal leaks. Careful posterior approach to the esophagus will assist stop recurrent laryngeal nerve damage, but dissection particularly to identify the nerve is discouraged as it might possibly increase the chance of nerve harm. A 29-year-old man is stabbed within the neck; throughout exploration you notice an esophageal as well as a tracheal laceration. Avoidance of drains to stop erosion in to repairs Most tracheal accidents could be closed primarily utilizing an absorbable suture in a single layer. Associated injuries of the thyroid or cricoid cartilage may be closed with sutures or plates. Esophageal accidents ought to be explored to ensure the whole mucosal defect is addressed. Intra-operative esophagoscopy and insufflation of a nasogastric tube with air or dye can aid within the analysis of suspected esophageal injury. Once the harm has been recognized it can be repaired in a single or two layers with absorbable suture. Conservative administration is an appropriate possibility within the secure patient with a contained perforation Timing of restore in esophageal injury is an important determinant of outcome, with delay 24 hours significantly decreasing possibilities of successful major repair and survival. Iatrogenic perforation is by far the most typical reason for esophageal harm; trauma accounts for 5�10% of injuries. Esophagoscopy is broadly utilized but could have 268 Surgical Critical Care and Emergency Surgery proven otherwise. Additionally, bradycardia and lack of response to fluid challenge make hemorrhagic shock less probably.
Purchase tetracycline 500 mg with mastercardOnly two of sixty three sufferers had transient urinary retention and there were no antagonistic occasions of bladder virus hitting us discount 500 mg tetracycline visa, bowel, vessel or nerve perforations, and no erosions, extrusions, muscle or groin pain. This short-term, potential analysis provides encouraging information that might need to be confirmed in bigger, potential research with longer follow-up. Needleless the Needleless System (Neomedic International, Terrasa, Spain) quietly emerged from Europe in 2007. The patented lateral pocket position- Results Despite being developed in 2007, scant peer-reviewed literature is out there for the Needleless sling. Based upon a negative cough test, a hundred sufferers (84%) were objectively cured, 10 (8%) improved their incontinence, and 10 (8%) had been thought of failures. The midline blue suture could be eliminated intraoperatively or left in place for publish operative changes (reproduced by permission of Neomedic International, Terrasa, Spain). Over the years, several Needleless abstracts have been presented at various worldwide society conferences. Mean operative time was 7 min (range 4�20 min) and hospital keep was eight h (range 4�24 h). Based upon objective and subjective measures, 69 patients (88%) achieved remedy of stress incontinence, four (5%) improved, and six (7%) failed. There were no instant complications; however, four partial erosions (5%) have been successfully managed with local estrogen remedy. Two sufferers had de novo urge incontinence and three had urge urinary incontinence managed with antimuscarinic brokers. All sufferers had urethral hypermobility and patients with neurogenic incontinence or intrinsic sphincter deficiency had been excluded. The imply age was fifty one years (41�70 years) and imply operative time 9 min (range 7�14 min). Complications included 5 momentary retentions, two nonintervention hematomas, and two partial sling extrusions treated with native estrogen therapy. Further multicenter research with longer followup have to be revealed to confirm the long-term effectiveness of this system. The Ajust polypropylene mesh sling features two anchors, one fixed and one adjustable, and is constructed with a suburethral section, as properly as a tubular adjustment mesh that slides in either path by way of the anchor. These mesh design features enable bidirectional impartial adjustment (tightening and loosening) of the sling mesh relative to the anchors with out visual obstruction from the introducer in the surgical field. After optimum sling rigidity setting, the flexible stylet is utilized to lock the sling in to place. The device is then inserted horizontally in the direction of the cephalad margin of the ischiopubic ramus, and pushed straight in to the obturator internus muscle. Once the mounted anchor passes the ischiopubic ramus, the surgeon should pause from the original push while pivoting the introducer deal with previous the midline, after which resume a second straight push maneuver to place the anchor fully through the obturator muscle and membrane. The midline indicator have to be deviated past the midline toward the fastened anchor side to confirm proper depth of placement. The mounted anchor is then released and traction is utilized to the suburethral portion of the sling to verify correct anchor engagement. The adjustable anchor is then loaded in to the Chapter 142 Single-Incision Slings 1681 introducer and the steps are repeated on the opposite aspect. Once the adjustable anchor is correctly positioned, the adjustment tab and tubular mesh is then pulled till the surgeon achieves the desired "set-point" of the suburethral sling. Once optimal setting has been achieved, the versatile stylet is used to advance the sling lock in to the adjustable anchor, locking it in place. The system is designed to allow post-anchor insertion bi-directional pressure adjustability (loosening and tightening) after the sling implantation with out additional insertion of the introducer. The anchoring in to the obturator membrane with bi-directional adjustability seems to have excellent preliminary subjective and objective success rates. Further potential studies with longer follow-up are needed to show the sustained sturdiness and efficacy. Nearly 50% of the surgeries have been done beneath local anesthesia and no concomitant prolapse surgery was performed. All procedures had been done in underneath 15 min with none intra- or post-operative problems. At a imply follow-up of 3 months, all 30 patients have been dry primarily based upon clinical examination, although one patient skilled delicate urgency. Forty sufferers acquired local anesthesia and had been managed on an outpatient foundation, whereas three patients had basic anesthesia and were hospitalized for twenty-four h. One affected person had a postoperative vaginal bleed and one had urinary retention efficiently managed with 1-day catheter drainage. The standardization of terminology of lower urinary tract operate: report from the standardization sub-committee of the international continence society. Challenge of One-incision midurethral sling for feminine stress urinary incontinence: Current outcomes. A three-year follow up of tension-free vaginal tape for surgical therapy of feminine stress incontinence. Prospective multicentre randomized trial of tension-free 1682 Section eight Lower Urinary Tract: Incontinence 25. Prospective evaluation of a single incision sling for stress urinary incontinence. Differential effects of cough, valsalva, and continence status on vesical neck movement. MiniArc single-incision sling system for female stress urinary incontinence: early outcomes. The MiniArc Sling System within the remedy of feminine stress urinary incontinence Neurourology 2009;35:334�343. Tension-free vaginal tape versus colposuspensions for primary urodynamic stress incontinence: 5-year observe up. The tension-free vaginal tape reviewed: an evidence-based review from inception to present status. Transobturator urethral suspension: miniinvasive procedure within the remedy of stress urinary incontinence in ladies. Novel surgical technique for the treatment of female stress urinary incontinence: transobturator vaginal tape inside-out. Transobturator sling for feminine stress incontinence with polypropylene tape and outside in process: prospective study with 1 year comply with up and review of transobturator tape sling. Multicenter expertise with the monarc transobturator sling system to deal with stress urinary incontinence. Retropubic compared with transobturator tape placement in therapy of urinary incontinence: a randomized controlled trial.
Prunus dulcis var. amara (Bitter Almond). Tetracycline. - Are there any interactions with medications?
- How does Bitter Almond work?
- What is Bitter Almond?
- Dosing considerations for Bitter Almond.
- Are there safety concerns?
- Spasms, pain, cough, itch, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96335
Tetracycline 500mg fast deliveryOpen prostatectomy for benign prosatic enlargement in southern Europe in the late 1990s: a recent sequence of 1800 interventions antibiotic jaw pain purchase tetracycline 500 mg line. Thulium:yttrium-garnet laser prostatectomy in males with refractory urinary retention. Photoselctive vaporization of the prostate: Subgroup analysis of males boundaries is an exciting instance of how primary physics finds its means in to clinical practice. Detailed knowledge of technical elements has lead to nice enhancements in laser units and consequently better medical remedy. Soft and hard tissue ablation with short-pulse high peak energy and steady thuliumsilica fiber lasers. High-power laser vaporization of the canine prostate using a 110 W Thulium fiber laser at 1. Thulium fiber laser lithotripsy: an in vitro evaluation of stone fragmentation using a modulated 110watt Thulium fiber laser at 1. Thulium laser resection of prostate-tangerine technique within the treatment of benign prostate hyperplasia. Holmium laser enucleation of the prostate: comparison on the effectivity measure at two institutions. Against the movement: Lasers are superfluous for the surgical management of benign prostatic hyperplasia in the growing world. Exvivo comparison of bipolar plasma-kinetic vaporization of the prostate to low power and high power Greenlight laser. Preliminary evaluation of a novel side-fire diode laser emitting gentle at 940 nm for the potential remedy of benign prostatic hyperplasia: ex-vivo and in-vivo investigations. Laser vaporization of the prostate: intermediate-term follow-up with the 200 W high-intensity diode (HiDi) laser system. Introduction of a novel method for the remedy of benign prostatic obstruction. Laser based mostly resecting methods within the remedy of benign prostatic obstruction. Retrograde blind endoureterotomy for subtotal ureteral stricture: a model new method. Thulium laser resection by way of flexible cystoscope for recurrent non-muscle-invasive bladder most cancers: initial clinical experience. Irrigation eliminates smoke formation in laser laparoscopic surgery: ex vivo results. These rely not only on the type of laser supply, laser applicator, and irradiation parameters, but additionally notably on the "therapy scheme". It can be performed using the same laser, applicator, and irradiation parameters, but resulting in a lowvolume coagulation. By distinction, in interstitial laser irradiation the applicator can be inserted in to the specified tissue as deep and as usually as necessary to coagulate any amount of tissue. Clinical outcomes, namely symptomatic enchancment, voiding parameter enchancment, and complications, rely not solely on surgical approach and strategy, but in addition on biologic motion. For unknown and unforeseeable reasons in some particular person cases, the necrotic tissue might stay in place, necessitating resection. Concomitant diseases, similar to strictures of the urethra or bladder calculi, may be handled in the same session. Patients with continual urinary retention or poor detrusor operate will need to have a catheter in place for a longer period after the process because of the time required for the prostate to shrink sufficiently to clear the obstruction. Virtually no intraoperative morbidity is related to interstitial laser remedy and in precept it can be performed with the affected person underneath local anesthesia (given that it seems acceptable to perform a cystoscopy with minor transurethral manipulation beneath native anesthesia) [6, 7]. Antegrade ejaculation was preserved in roughly 80% of sufferers who underwent the laser process [13�18]. The surgeon can increase this chance by not treating the bladder neck; however, this carries the chance of a suboptimal correction of voiding signs. In any case, the affected person ought to be suggested that the loss of prograde ejaculation is a potential aspect effect of interstitial laser remedy. Patients with obstructive symptoms from carcinoma of the prostate are also candidates for interstitial laser therapy [20]. However, interstitial laser remedy is certainly not an different choice to radical prostatectomy or healing radiotherapy. If curative therapy is possible, a screening biopsy ought to be carried out and evaluated earlier than laser treatment. Routine perioperative antibiotic prophylaxis is beneficial [14] to produce sterile urine preoperatively, notably if a prostate biopsy is to be performed transrectally on the time of laser therapy. Additional urodynamic measures (pressure�flow studies) are useful for assessing the lower in obstruction after laser therapy. As for other procedures, informed consent ought to embrace information about the totally different remedy options, together with transurethral resection, and the particular advantages, disadvantages, dangers, and potential complications of every technique. The likelihood of the affected person retaining regular sexual operate is approximately 80% [22, 23]. The patient ought to be aware that the failure rate for this process is about 10�15% inside 1 12 months (for an unselected group of patients) and that postprocedure catheterization (permanent or intermittent [24]) will be essential for some time. The affected person ought to know that at present the longest follow-up is just 10�12 years and publications on long-term outcomes are available for follow-up of four, 5, and 7 years solely [25�27]. Some risks can only be theorized, corresponding to coagulation of the rectum with consequent fistulas, damage to the Preoperative preparation Interstitial laser therapy may be performed with an area [6, 7], regional, or systemic anesthetic. If native anesthesia is chosen, such as by transperineal injection of lidocaine to achieve a blockade of the prostate and pudendal nerves, overfilling of the bladder, which could cause discomfort, ought to be averted. Although no everlasting irrigation is necessary throughout this procedure, a suprapubic catheter could be helpful. After enough anesthesia is induced, the patient is positioned within the dorsal lithotomy position. Routine disinfection and a noninflammable drape, as typically required for any laser surgery, ought to be used. Interstitial laser applicators may be positioned using a quantity of totally different approaches [16, 30]. In practice, endoscopically-controlled transurethral placement has proved most helpful. Instrumentation Several laser wavelengths have been studied to be used in interstitial laser therapy [10�12, 28, 31�35]; printed stories have demonstrated that 800�1100-nm wavelengths offer comparatively deep penetration depths in water and efficient volumetric heating, which enable the delivery of necrotic temperatures deep in to tissues. Even with low-laser energy, high-power Chapter a hundred thirty Interstitial Laser Therapy 1561 densities are achieved (330 W/cm2 with 1 W), resulting in quick carbonization and vaporization. Experiments have demonstrated that interstitial irradiation with a naked fiber at as a lot as a 20-W energy setting produces only a small spherical lesion of 5�10 mm diameter, consisting of a central cavity filled with particles, and adjoining char and a small coagulated rim [30, 38�40, forty nine, 50�55]. To avoid charring and to achieve large-volume coagulation, the power density of an interstitial applicator must be a lot lower (5�10 W/cm2) [40, 56]. Since Bown first discussed interstitial laser therapy for most cancers treatment in 1983 [57], a number of types of applicators with larger irradiating surfaces have been used in laboratory or medical experiments [35, 53, 58�65], but these have all produced similarly unimpressive outcomes.
Discount tetracycline amexProper infiltrative strategies virus list purchase tetracycline 250 mg with amex, together with a fundamental data of the surrounding anatomy and aspiration previous to injection of the anesthetic, help to keep away from these problems. Cardiovascular side effects range from bradycardia, atrioventicular block, and ventricular arrhythmias to cardiac arrest [15]. Amide anesthetics are metabolized by the liver and excreted by the kidneys, so the dosage must be decreased in sufferers with either liver or kidney failure [13]. As such, oral pain medicines, sedatives, and antianxiety medicines are often considered together with anticholinergics. The use of oral medicines, while probably very useful to sufferers, has not been studied in a means that enables "best practices" to be established. It may be safely stated that the preoperative medicines used are usually very well understood by urologists, who use comparable medicines in the day-to-day management of their patients (Table 123. Nevertheless, preoperative oral drugs that add to patient consolation and safety are clearly applicable. In basic, 10�30 mL of 2% lidocaine gel is instilled for a 5�20 min dwell time previous to the particular process. If indeed lidocaine gel is nothing greater than a placebo, it may be a priceless placebo. Topical urethral anesthesia Prior to flexible cystoscopy being out there, urologists routinely performed inflexible diagnostic cystoscopy within the office with or with out an anesthetic gel, corresponding to 2% lidocaine. Urologists experienced with rigid cystoscopy understood that a lot of the discomfort tended to happen as the scope traversed the membranous and prostatic urethra, straightening the bulbous and proximal urethral anatomy. Patients reflexively resist cystoscopy by tightening the perineal musculature and membranous urethra. However, as soon as within the bladder, sufferers would typically loosen up with the words "the worst half is over". Again, patient choice was nonetheless very important in enhancing the chances of a profitable process. Though lidocaine gel has been used for decades for cystoscopy in males, the proof that it actually works properly as an area anesthetic is lacking. They discovered a barely vital distinction in affected person perceived pain scores [17]. There are numerous fashionable studies suggesting that 2% lidocaine works no higher than water-soluble lubricant for flexible cystoscopy in the male [18�22]. It is likely that very little lidocaine is definitely delivered to the prostatic urethra or is ready to dwell there. Normal retrograde urethrograms seldom present a lot contrast in the prostatic urethra. Though intravesical lidocaine has been used as a neighborhood anesthetic for bladder procedures, it has not been suggested as a prostatic anesthetic [23, 24]. These endoscopic procedures should be carried out with clear visualization of the prostatic urethra for optimum performance. Any sudden motion of the affected person can jeopardize the procedure because of bleeding or patient discomfort. As such, all procedures were initially developed underneath common, regional (spinal) or intravenous sedation. Urologists experienced with prostate blocks for prostate biopsy and transurethral needle injection approach started to develop methods to block the posterior urethra and prostate in such a way that these procedures could presumably be performed within the workplace setting. They were motivated to develop their very own in-office protocols in the hope of saving general prices with out diminishing physician reimbursement. There are, however, articles on native prostate block for prostate procedures and much has been written on local anesthesia for prostate biopsy. Moffat injected 10 mL of 1% lidocaine with epinephrine in to each lobe of the prostate of 18 patients through a digitally-guided transperineal route utilizing a 20G spinal Chapter 123 Local Anesthesia for Minimally Invasive Treatment of the Prostate in the Office Setting needle [27]. Remarkably, eight of the 18 patients had no intravenous sedation and no preoperative drugs got. The sufferers apparently acquired no supplemental preoperative or intraoperative drugs. These examples recommend that local prostate block can allow for major endoscopic prostate procedures and that the block itself is liable for ache control as opposed to oral or parenteral supplements. Prior to transrectal prostate ultrasound, digitally-guided transrectal biopsy of the prostate was routinely carried out with acceptable affected person tolerance utilizing no anesthetic. Subsequent studies instructed that ultrasound-guided transrectal lidocaine on the apex labored just as well or better [33�36]. Transrectal intraprostatic injection of the prostate has been instructed as better than a periprostatic block for ache management [37]. Finally, a periprostatic and intraprostatic mixture block may go best of all for transrectal ultrasoundguided biopsies [38, 39]. The incidence of febrile episodes after transrectal prostate biopsy may be rising. Efforts ought to be made to make positive the rectal vault is empty of stool previous to biopsy and prophylactic antibiotics should be given. The commonplace method calls for ultrasound-guided injection of no much less than 5 mL of 1% lidocaine in to the fats plane seen laterally at the base of the prostate, between the seminal vesical and rectum. On sagittal view, this seems as a "triangle," referred to by Jones because the "Mount Everest sign" (see Video 123. Alternatively, or on the same time, 5 mL of 1% lidocaine could be injected in to the periapical fats, deep and lateral to the apex, between the prostate and rectum. On sagittal view, infiltration of anesthetic may be seen to separate a tissue plane that programs in direction of the base [33, 36]. The article by Berland and Jones in e-medicine absolutely describes transrectal periprostatic blocks and is a useful web site. Using the same ultrasound-guided approach, intraprostatic anesthesia can be delivered by injecting 10 mL of lidocaine in increments in two to three websites within every lobe of the prostate from apex to base [37]. Kedia used a digitally-guided transrectal lidocaine block to perform interstitial laser coagulation of the prostate [41]. Other than transurethral lidocaine (a liquid and gel), patients received no oral or parenteral medications apart from antibiotics. He claims to not have terminated or abbreviated any procedures in over 300 cases (personal communication). Members of our group are performing laser (Evolve and Green Light) procedures utilizing transrectal ultrasound guided periprostatic and intraprostatic blocks with lidocaine. Good functional outcomes had been lately presented at our State Urological Society Meeting [43]. Unlike the transrectal method, the chance of an infection ought to be lessened by permitting for a correct pores and skin preparation and directing the needle to keep away from contamination from the rectal mucosa. The affected person is positioned in the dorsolithotomy place with the perineum prepped and draped. A 27G needle could additionally be used to anesthetize the entry site within the perineum above the perineal physique. The needle is directed in to the midline, deep to the apex of the prostate beneath transrectal digital steerage.
Generic 500 mg tetracycline amexSigns of sympathomimetic toxidrome are hypertension antibiotic resistance virtual lab buy generic tetracycline 500mg on line, tachycardia, mydriasis, and diaphoresis. Sedative/hypnotic toxidrome is mirrored by confusion, stupor, slurred speech, and apnea. A 25-year-old woman ingested 10 tablets of carisoprodol 350 mg, 30 tablets of ibuprofen 200 mg and 10 tablets of cephalexin 500 mg 2 hours ago. Gastric lavage There is little proof that any technique of gastric decontamination is of benefit in overdose patients, nevertheless, activated charcoal is the best response. Activated charcoal adsorbs most ingested medication and is mostly effective and well tolerated. Whole-bowel irrigation could additionally be used in intoxications the place activated charcoal is ineffective. It is considered for medication such iron, lithium, sustained-release agents and illicit drug packets. This results in accumulation of natural acids, corresponding to lactic acid and ketoacids, and metabolic acidosis with an elevated anion hole. Which one of the following options of salicylate toxicity or remedy of salicylate toxicity is inaccurate: A. The toxidrome for salicylates includes nausea, vomiting, dyspnea, diaphoresis, dizziness, and tinnitus B. Significant ingestions of salicylates result in respiratory acidosis or combined metabolic alkalosis and respiratory acidosis C. Activated charcoal is beneficial for acute salicylate ingestions, but not in circumstances of toxicity from continual exposure the salicylate toxidrome includes nausea, vomiting, dyspnea, diaphoresis, dizziness, and hearing changes. Poisoned sufferers suffer from respiratory alkalosis or mixed anion-gap metabolic acidosis and respiratory alkalosis. Pulse oximetry precisely reflects oxygen saturation as a outcome of it might possibly distinguish carboxyhemoglobin from oxyhemoglobin C. Higher carboxyhemoglobin concentrations (10�30%) cause headache, dizziness, dyspnea, irritability, nausea, and vomiting. Administration of 100% supplemental oxygen decreases the half-life of carboxyhemoglobin from 5�6 hours to 45�90 min. She is chronically handled with lithium however had an ingestion of numerous sustained-release lithium roughly four hours prior to admission. The biggest risk of lithium ingestion is central nervous system toxicity together with delirium, tremor, ataxia, hyperreflexia, seizures and coma. Lithium is a prototypical dialyzable agent because of its low molecular weight, lack of protein binding and extended half-life (18 hours). The stage will be decreased successfully by hemodialysis; nevertheless, repeat ranges should be obtained after dialysis to assess for rebound increase as lithium shifts from the intracellular to extracellular area. Volume replacement is appropriate in these patients as a end result of lithium causes a nephrogenic diabetes insipidus. Methanol is metabolized by alcohol dehydrogenase to formaldehyde, which is then transformed to formic acid. Accumulation and precipitation of calcium oxalate crystals within the renal tubules that leads to the development of acute tubular necrosis occurs after ethylene glycol ingestion. Fomepizole and ethanol are inhibitors of alcohol dehygrogenase (not inducers) and thus, inhibit the formation of poisonous metabolites of both substances. Metabolic acidosis with an elevated anion hole and an elevated osmolar gap are traditional options of nonethanol intoxication. Late presentations may not manifest an osmolar hole if the alcohol has already been metabolized to acid metabolites, however an anion gap acidosis will be apparent. Ethylene glycol is metabolized by alcohol dehydrogenase to formaldehyde and then to formic acid B. Accumulation and precipitation of oxalic acid to calcium oxalate within the renal tubules produces crystals and contribute to the development of renal tubular necrosis after methanol ingestion C. The remedy of choice for ethylene glycol and methanol poisoning is to enhance elimination of metabolites by administering fomepizole or ethanol which induces the alcohol dehydrogenase enzyme E. These ingestions are rare however can end result in important morbidity and mortality. Ethylene glycol is metabolized by alcohol dehydrogenase to glycoaldehyde and glycolic acid and then finally to glyoxylic acid and oxalic acid. These papers function as scientific apply guidelines for elimination strategies for poisoned sufferers. However, it ought to be considered if the toxin is thought to be adsorbed by charcoal and has been ingested within 1 hour. Administration of multidose activated charcoal should be thought of for patients which have ingested life-threatening amounts of carbamazepine, dapsone, phenobarbital, quinine, or theophylline. A 66-year-old overweight man who was lately discharged from the inpatient medical service is found down by his wife with a small hematoma on his scalp. His physical examination is unremarkable aside from the small cephalohematoma and his trauma workup is unfavorable. Severe, extended hypoglycemia is attribute of Envenomations, Poisonings and Toxicology ingestion of enormous doses of sulfonylureas. Sulfonylurea agents stimulate insulin launch from the pancreas, resulting in hypoglycemia. Risk factors for hypoglycemia from therapeutic use include: age sixty five years, a number of drugs, frequent hospitalizations, use of brokers with longer durations of motion. Octreotide is a somatostatin analogue that inhibits launch of insulin from the pancreas and has been discovered to be efficient in treating hypoglycemia and shortening the period of hypoglycemia. The most essential mechanism of action is G-protein-mediated lower in calcium inflow by way of voltage-gated channels in pancreatic beta islet cells, which diminishes calciummediated insulin release. The dose of octreotide is 50 to 150 g administered by intramuscular, or subcutaneous, injection each six hours. The efficacy of glucagon is dependent upon hepatic glycogen shops, which can be depleted in the setting of extended hypoglycemia. Central venous entry is required for administering concentrated glucose solutions because of hyperosmolarity that can trigger endothelial damage. The affected person had been dropped at the emergency department for evaluation by some pals after mountaineering. His bodily examination is outstanding for bleeding gums and an ecchymotic, edematous left lower extremity from foot to knee with a small wound near the ankle. Which one of many following interventions could be most useful to this patient Administration of Crotalinae (pit viper) antivenom (Polyvalent Crotalidae ovine immune Fab) E. Fasciotomy of the left lower extremity the physical findings on this patient are regarding for compartment syndrome.
References - Daliani DD, Tannir NM, Papandreou CN, et al. Prospective assessment of systemic therapy followed by surgical removal of metastases in selected patients with renal cell carcinoma. BJU Int 2009;104(4):456-460.
- McKinney AM, Short J, Truwit CL, et al. Posterior reversible encephalopathy syndrome: incidence of atypical regions of involvement and imaging findings. AJR Am J Roentgenol 2007; 189:904-12.
- Klein J, Zhuang Z, Lubensky I, et al. Multifocal microcysts and papillary cystadenoma of the lung in von Hippel- Lindau disease. Am J Surg Pathol 2007;31:1292-6.
- Christ-Crain M, Jaccard-Stolz D, Bingisser R, et al. Effect of procalcitonin-guided treatment on antibiotic use and outcome in lower respiratory tract infections: cluster-randomised, single-blinded intervention trial. Lancet 2004; 363: 600-607.
- Maiorana A, Ficarra G, Fano RA, Spagna G. Primary solitary meningioma of the lung. Pathologica 1996;88(5):457-62.
|


