|
Valerie L. Katz, MD, FACS - Assistant Professor of Clinical Surgery
- Weill Medical College of Cornell University
- Section Chief, Department of General Surgery
- Lincoln Medical and Mental Health Center
- Bronx, New York
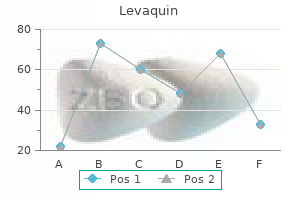
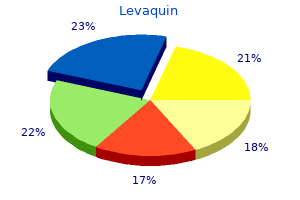
Levaquin dosages: 750 mg, 500 mg, 250 mg
Levaquin packs: 60 pills, 90 pills, 120 pills, 180 pills, 360 pills

Order levaquin online from canadaIn addition to tubal function exams medications heart failure 500mg levaquin sale, these teams ought to be evaluated for risk elements when a continual perforation is present (immunologic standing, allergy, adenoid hypertrophy, and social and environmental factors). In Chapter 10, I described a sequence of occasions that I consider leads to continual suppurative otitis media. The study that reported these microbiologic findings was not associated to continual perforations but somewhat acute otitis media with otorrhea when tympanostomy tubes were in place67; thus, a future goal can be to carry out middle-ear cultures when an acute assault of otorrhea happens when a tympanic membrane perforation is present. The subsequent step would be to confirm the hypothesis that organisms isolated from persistent otorrhea. Although a related query may be obvious, my competition is that should you deal with acute otitis media with otorrhea effectively, chronic otorrhea is prevented. Even though we initially advocate intravenous remedy for these patients and carry out a tympanomastoidectomy only for those people who fail to respond, this apply relies on an empiric foundation and not from evidence-based medicine. Some clinicians recommend adenoidectomy for sufferers who develop continual suppurative otitis media in an effort to treat the continual an infection and forestall recurrence, however no clinical trial has been reported that addressed this query. In addition, management of these problems is predicated on empiric selections and never on evidence-based scientific trials. If so, should their management differ relying on the presence or absence of effusion No randomized medical trials have been reported that have adequately answered these essential scientific questions. A scientific trial of insufflation of a corticosteroid into the tube and middle ear appears to be an appropriate therapy for assessment. Even though inflation with air into the center ear was reported to not be effective in a single study,seventy two future trials utilizing a different methodology (or gas) could additionally be efficient. No clinical trials have addressed the efficacy of surgery to prevent progression of the atelectasis (with or without retraction pocket) in an try to stop a cholesteatoma from developing. The question is what are the indications for tympanostomy tube placement or tympanoplasty, or both procedures, related to length, severity, extent, the age of the affected person, and different factors We did take a look at the operate of the tube in a few kids with congenital cholesteatoma years ago, which we thought was inside regular limits, however that is an attention-grabbing and potentially necessary medical analysis query. An necessary unanswered clinical question is which operative procedure is the safest and best to eradicate in depth cholesteatoma Both the closed-cavity canal wall up tympanomastoidectomy, with tympanoplasty, and canal wall down mastoidectomy are at present carried out around the world for in depth cholesteatoma. Recurrent and persistent otorrhea is unusual following an intact canal wall mastoidectomy with tympanoplasty (the fuel cushion is maintained). Randomized medical trials addressing the unanswered clinical query of which procedure is the most secure and most effective, with a minimum of long-term postoperative care and issues, corresponding to troublesome otorrhea, are future research goals. If this could be profitable, the patient should have a extra physiologic middle ear�mastoid system. It has been instructed that congenital cholesteatoma could also be acquired (secondary to otitis media). Onset of otitis media within the first eight weeks of life in Aboriginal and non-Aboriginal Australian infants. Prevalence of otitis media in chosen populations on Pohnpei: a preliminary examine. Screening for otitis media with effusion to measure prevalence in Chinese children in Hong Kong. Effect of surgical alteration of the tensor veli palatini muscle on Eustachian tube function. Measurement of Eustachian tube mechanical properties utilizing a modified pressured response check. Eustachian tube closing failure: incidence in patients with cleft palate and middle-ear disease. Eustachian tube compliance in sniff-induced otitis media with effusion: a preliminary study. On the physics of the toddler feeding bottle and middle-ear sequela: ear disease in infants could be associated with bottle-feeding. A double-blind, placebocontrolled, medical trial of the impact of chlorpheniramine on the nasal airway, center ear and Eustachian tube to provocative rhinovirus challenge. Otologic and systemic manifestations of experimental influenza A virus infection within the ferret. Nasal and otologic results of experimental respiratory syncytial virus infection in adults. Magnetic resonance imaging of the event of middle-ear effusion secondary to experimental paralysis of tensor veli palatini muscle. In vivo remark with magnetic resonance imaging of middle-ear effusion in response to experimental underpressures. Eustachian tube histopathology during experimental influenza A virus infection within the chinchilla. Daily tympanometry in youngsters in the course of the chilly season: association of otitis media with higher respiratory tract infections. Effect of floor rigidity and surfactant administration on Eustachian tube mechanics. Point prevalence of barotitis and its prevention and remedy with nasal balloon inflation: a potential, managed research. Recent advances in otitis media with effusion: proceedings of the Second International Symposium. Comparison of Eustachian tube function checks between youngsters with cholesteatoma/retraction pocket and people with continual otitis media with effusion. Index Page numbers adopted by "f " and "t" indicate a figure and a table respectively. Jan Danser, and Jeroen Essers Content Introduction 5 Structure of the vascular wall 6 Components of the vascular wall 8 Types of blood vessels 11 Ageing and the vascular wall 14 Summary 16 Introduction A healthy heart pumps about 6,000�8,000 litres of blood across the physique every day. Pulmonary circuit: the proper ventricle of the heart pumps blood into the lungs, the place waste gases are exchanged for oxygen, after which the blood is transported again to the left atrium of the center. Systemic circuit: the left ventricle pumps oxygenated blood to all tissues and organs of the physique by way of the aorta, after which deoxygenated blood is transported back to the right atrium of the guts. Rather, it refers to a lower oxygenation grade than that of oxygenated blood as a end result of a certain amount of oxygen has been delivered to tissues. As a end result, deoxygenated blood still incorporates about 75% of oxygen in comparability with oxygenated blood. The blood vessels are a conduit for a wide selection of molecules, similar to vitamins, oxygen, and waste products, to and from all elements of the physique. Structure of the vessel wall Pulmonary circuit To the center Heart From the heart Blood vessels have to be well-constructed, as they need to withstand the stress of circulating blood by way of the physique daily. These layers primarily include endothelial cells, vascular clean muscle cells, and extracellular matrix, together with collagen and elastic fibres. In wholesome vessels, it consists of a thin single layer of endothelial cells, that are in direct contact with the blood within the lumen, as properly as a subendothelial layer made up principally by connective tissue. The single layer of endothelial cells, referred to as endothelium, has a clean floor that minimizes the friction of the blood because it strikes by way of the lumen. The endothelium plays a job in vascular permeability, inflammation, coagulation, and vascular tone, which refers to the maximal diploma of contraction by vascular smooth muscle cell relative to its maximally dilated state.
Buy levaquin 750 mg without a prescriptionSpecifically treatment laryngitis order levaquin 250mg free shipping, sluggish (viscous) deformation based on a sliding-filament mechanism of the two-fold helix of the glycan (49) might vascular wall 37 clarify the massive portion of macroscopic viscoelasticity seen in arterial tissues. In vitro testing of vascular tissue sometimes displays pronounced stress softening under the first few loading cycles. Vessels exhibit a nearly repeatable cyclic behaviour as quickly as stress softening is full, i. Mechanical damage and failure effects Mechanical pressure is transmitted from the macroscopic (tissue) length-scale all the method down to the atomistic length-scale, and completely different microstructural constituents are loaded differently. Consequently, raising the macroscopic load results in local stress concentrations within the tissue, and, if excessive enough, begins damaging it at particular spots. For example, micro-defects, such as breakage and pull-out of collagen fibrils, progressively develop, which in turn weakens the tissue. In vitro supra-physiological inflation (51) signifies that softening and plastic phenomena could interfere with one another, and there may be some relation between preconditioning and damage-related phenomena (52, 53). Stress and strain state within the vessel wall Wall stress and strain are the mechanical responses to exterior forces appearing on the vessel and are distributed in a different way all through the vessel layers. This equation can only be solved analytically (exactly) for a only a few, rather simple issues. However, this homeostatic target can clearly not be maintained in diseased vessels, and, in an aneurysm wall, for instance, the strain can reach a number of hundred occasions this value. The adventitia is encompassed repeatedly by unfastened connective tissue that anchors the vessel to its surrounding. Despite the truth that this describes probably the most basic approach of blood/vessel wall interaction, sub-classes of issues with explicit options are known for particular applications; a few of them are mentioned here. At physiological loads, only 6% to 7% of collagen fibres are engaged (57, 41), such that vascular tissue can address a lot larger stresses than physiological ones previous to mechanical failure. Wave propagation the elastic vitality saved in vessels coupled to the mass of blood (and tissue) outline the bodily circumstances for propagating pulse waves. Different techniques for the in vivo measuring of the heartbeat wave velocity are identified (8), such that vessel stiffness can be non-invasively estimated with the help of the Moens� Korteweg equation. Vessel tissue modelling In order to analyse bodily processes in the vasculature, constitutive fashions for vascular tissue are required. The literature on such constitutive fashions is wealthy and the level of modelling is strongly linked to the target of the biomechanical computation. Specifically, hyperelastic models (43, fifty eight, fifty nine, 36), pseudoelastic fashions (48), viscoelastic models (60), poroelastic fashions (61), viscoplastic fashions (53), and damage models (62) are all current in the literature. Constitutive models of the arterial wall, or layers of it, are either primarily based on a purely phenomenological method (43, 58) or take structural info of the underlying histology under consideration (36, 59, sixty three, sixty four, 65). Vascular tissue is a dynamical construction whose mechanical properties adapt to adjustments in its setting. Consequently, a category of constitutive descriptions aims at addressing the turnover of key vascular constituents (64, sixty seven, 68). Permeability A pressure gradient exists between the arterial circulation and the interstitial stress in the adventitia, generating a transmural fluid move radially outwards by way of the arterial wall. This hydraulic conductance from the lumen to the adventitia conveys substances that can be retained, modified, and activated throughout their mass transport through the wall (1). In the vasculature, permeability is intently related to the endothelial layer that facilitates a selective transport of small molecules (ions, water, and nutrients) and even entire cells (lymphocytes) out and in of the vessel (72). Consequently, the endothelium is a semi-selective barrier between the vessel lumen and surrounding tissue, Blood/vessel interplay Vascular structure interferes with blood move and vice versa, either by energetic contraction of the center muscle or just by a passive mechanical response to the pulsating circulate in larger arteries, for example. Originally, this relation was experimentally derived by Darcy, however it also follows from the equilibrium equation (3. Despite the truth that mixture theory is more common than poroelasticity, by providing higher conceptual mechanisms to integrate physical situations (80), poroelasticity was just lately extended to mannequin blood flows via the beating myocardium, for instance (81). Cardiovascular perform critically is decided by the right mechanical interplay between blood and the vessel wall, and haemodynamics-based biomechanical elements of the cardiovascular system are a standard denominator of cardiovascular pathologies. When offering enter info, such as three-dimensional geometry or blood velocities on the boundaries of the computational domain, such tools synergetically mix with modern picture modalities. However, shut interaction between engineering and medical disciplines is crucial to the profitable exploration of the related physical phenomena. Consequently, tissue deformation interacts with interstitial circulate and vice versa, phenomena that can be studied by the theories of mixtures and poroelasticity. The principle of mixtures relies on diffusion fashions (75�78) whereas poroelasticity models the interaction of deformation and fluid move in a fluid-saturated porous, elastic medium Further reading B�ck, M. An Introduction to Continuum Mechanics, Cambridge University Press, New York, 2013. Role of endothelial shear stress within the pure history of coronary atherosclerosis and vascular reworking: Molecular, cellular, and vascular behavior. Effects of elevated plasma viscosity and pink blood cell aggregation on blood viscosity in vivo. An optimization strategy for oblique indentification of cohesive crack properties. Computer simulation of local blood circulate and vessel mechanics in a compliant carotid artery bifurcation mannequin. Three-dimensional simulation of blood move in an belly aortic aneurysm-steady and unsteady flow cases. Using image-based large-eddy simulations to investigate the intracardiac flow and its turbulent nature. Method for the calculation of velocity, rate of move and viscous drag in arteries when the pressure gradient is known. Velocity profiles of oscillating arterial flow, with some calculations of viscous drag and the Reynolds quantity. Synergy between shear-induced migration and secondary flows on pink blood cells transport in arteries: concerns on oxygen transport. An built-in fluidochemical mannequin towards modeling the formation of intra-luminal thrombus in abdominal aortic aneurysms. The impact of age on the unfolding of elastin lamellae and collagen fibers with stretch in human carotid arteries. The static elastic properties of 45 human thoracic and 20 abdominal aortas in vitro and the parameters of a new model. Hyperelastic modelling of arterial layers with distributed collagen fibre orientations. Experimental investigation of the distribution of residual strains within the artery wall. Viscoelasticity and preconditioning of rat skin beneath uniaxial stretch: microstructural constitutive characterization.
Cheap 500 mg levaquin with amexThe membrane would then lose elasticity and would turn out to be retracted and denivit intensive treatment discount 250 mg levaquin fast delivery, ultimately, atelectatic. Inflammation between the medial portion of the retracted or collapsed tympanic membrane might then end in adhesive changes and could repair the pocket to the ossicles, surrounding constructions, or each. The next stage in this collection of occasions would be discontinuity of the ossicles or cholesteatoma formation, or both. It is incessantly difficult to distinguish between a deep retraction pocket and a cholesteatoma in both the posterosuperior quadrant of the pars tensa or the pars flaccida, even with assistance from the otomicroscope. The transition between the two circumstances often follows a progressive change from a retraction pocket to cholesteatoma; however, the factors concerned on this transition are currently obscure, although infection within the retraction pocket sac seems to be important. As described earlier, a typical sequela of middle-ear illness in patients with a cleft palate is cholesteatoma. In distinction to the frequency of cholesteatoma within the cleft palate population, cholesteatoma is rare in American Indian populations. This kind of tube would most likely preclude the event of high negative middle-ear stress, a retraction pocket, or cholesteatoma. The Apache Indian seems to have a tube that permits for easier passage of gas and liquid than does the white individual with or without a cleft palate. By finding out these in vivo models, we are in a position to achieve a clearer perspective of the entire spectrum of tubal dysfunction (see Chapter 6). Surgery Related to Dysfunction of the Eustachian Tube System When a cholesteatoma is current, surgical intervention is indicated. The determination as to the most appropriate surgical administration for cholesteatomas ought to be tailored for the individual patient. A second-stage exploratory tympanotomy should be thought of 6 months after the initial process to uncover residual disease. This time interval 210 is somewhat shorter than that advocated for adults, but residual cholesteatoma grows more quickly in youngsters than in adults. Rosenfeld and colleagues reported that unsuspected residual cholesteatoma was identified during 21 (39%) of fifty four second-look procedures in our review of 426 procedures. The use of the 70-degree telescope can be helpful in determining whether cholesteatoma is within the sinus tympani and facial recess through the preliminary operative process and at the time of the second-look exploratory tympanotomy. In many instances, the surgery could be restricted to the middle ear when the cholesteatoma entails only the middle ear. Because a retraction pocket cholesteatoma is secondary to chronic irregular unfavorable middle-ear stress, placement of a tympanostomy tube on the time of the original surgery may be useful in stopping recurrent illness at the identical or a different site. But cartilage graft tympanoplasty is an alternate if no middle-ear effusion is current (see Tympanoplasty). The granuloma within the mastoid may be eliminated by performing a complete simple mastoidectomy, and the center ear portion can be eliminated by using a tympanomeatal approach. From what is known of the pathogenesis of ldl cholesterol granuloma, one of the best administration is prevention, which should include offering regular aeration of the middle ear. This may require the position of tympanostomy tube, even a everlasting one, as a result of the disease is frequently recurrent. Middle-ear disease in distant Aboriginal Australia: a area evaluation of surgical outcomes. This sequela of middleear illness is uncommon in all age teams however does occur in children. These investigators concluded Role in sure problems and Sequelae of middle-Ear Disease 11. Results of tympanoplasty and mastoidectomy on the Massachusetts Eye and Ear Infirmary. The prognostic worth of Eustachian tube perform measurements in tympanoplastic surgery. Epidemiology and pathogenesis of chronic suppurative otitis media: implications for prevention and treatment. Bacterial colonization of the nasopharynx predicts very early onset and persistence of otitis media in Australian Aboriginal infants. Patterns of persistent otitis media in the first year of life in Aboriginal and non-Aboriginal infants. Mechanics of the Eustachian tube because it influences susceptibility to and persistence of 211 32. Medical management of continual suppurative otitis media without cholesteatoma in children-update 1992. Recent advances in otitis media-proceedings of the Fourth International Symposium. Aeration: an element in the sequelae of persistent ear disease alongside the Labrador and Northern Newfoundland coast. Otitis media in Alaskan Eskimo children: prospective analysis of chemoprophylaxis. Comparison of Eustachian tube function tests between youngsters with 212 cholesteatoma/retraction pocket and those with continual otitis media with effusion. Proceedings of the Third International Conference on Cholesteatoma and Mastoid Surgery. Variability of Eustachian tube function; comparison of ears with retraction disease and normal ears. Organic change of effusion within the mastoid in otitis media with effusion and its relation to attic retraction. Tympanic membrane vibrations in human cadaver ears studied by time-averaged holography. Functional Eustachian tube obstruction in acquired cholesteatoma and related conditions. The effect of nasal steady constructive airway pressure on regular ears and on ears with atelectasis. A model to clarify the speedy strain decrease after air-inflation of diseased middle ears. Zur Entstehung des Cholesteatoms des Mittelohrs (Cysten in der Schleimhaut der Paukenhohle, Atrophie der Nerven in der Schnecke). Cholesteatom, Perforation der Membrana Flaccida Shrapnelli und Tubenverschluss, eine Atiologische Studie. Pathogenesis of attic cholesteatoma: scientific and immunochemical support for combination of retraction concept and proliferation principle. Roentgenographic evaluation of the Eustachian tube operate in infants with cleft and normal palates. A comparison of cartilage palisades and fascia in tympanoplasty after surgery for sinus or tensa retraction cholesteatoma in children. Eustachian tube dysfunction in the pathogenesis of cholesteatoma: clinical considerations.
Buy 250mg levaquin with mastercardThe most typical result of a dysfunction of the system is growth of middle-ear underpressures medications xyzal buy cheap levaquin 750 mg, which might progress into middle-ear disease. The middle ear and mastoid can be contaminated by two main routes: reflux of infected secretions from the nasopharynx or contamination of the middle-ear cleft from the external auditory canal, mostly from water within the ear canal. But dysfunction of the tubal system is most frequently the cause of underpressures growing in the center ear, which may progress to middle-ear disease. Because middle-ear irritation can obstruct the osseous portion of the tube, preventing sufficient pressure regulation of the center ear (anatomic obstruction at the middle-ear end of the system, which might impair the pressure regulatory and clearance capabilities of the tube), secretions are trapped within the center ear. From my description of the inverted flask in Chapter 5, as liquid flows down the narrow neck, unfavorable strain develops in the bulbous portion of the flask. From knowledge of fluid dynamics via a collapsible tube, liquid flows extra readily than gasoline. Thus, if optimistic pressure has been recognized within the middle ear throughout these occasions, nasopharyngeal secretions are much more more probably to be forced into the center ear. Abnormalities of the system which are a main cause are as a result of either anatomic or functional obstruction of the tube or both. Anatomic obstruction is most incessantly attributable to inflammation, which is mostly viral in etiology. Evidence for viruses as the cause for tubal dysfunction and middle-ear adverse strain has been demonstrated in studies that involved adult volunteers; nevertheless, as described subsequently, topics who had preexisting tubal dysfunction were at highest risk of developing middle-ear underpressures after being challenged with a respiratory virus inoculated into the nasal cavity. Development of underpressures within the center ear could presumably be from any of the intrinsic or extrinsic anatomic situations that are related to pathophysiology of the tube itself (such as allergic inflammation); at either finish of the tubal system, similar to obstruction on the nasopharyngeal finish, as could be brought on by adenoids or tumor; or at the middle-ear end of the system, such as cholesteatoma or polypoid granulation tissue. Functional obstruction of the tube inside its system can even trigger main improvement of middle-ear negative stress. The potential underlying causes of functional obstruction of the tube are introduced in Chapter 5 however embody a floppy cartilage, dysfunction of the tensor veli palatini muscle, and constriction of the tube throughout swallowing. As postulated by Politzer, middle-ear negative pressure may cause transudation of fluid from the middle-ear mucosa into the cavity of the center ear. Since his time, subsequent observations and now studies in people and animals have provided proof to assist his hydrops ex vacuo principle. But as proven subsequently, following intranasal inoculation of a virus in an adult volunteer, tubal obstruction occurred, followed by middle-ear unfavorable underpressure and the subject creating an attack of acute viral and bacterial otitis media. Before and periodically after this nasal problem, assessments were manufactured from tubal function (using sonotubometry and the nine-step test), middle-ear stress (using tympanometry), and nasal patency (using lively posterior rhinometry). All outcomes completely resolved within 16 days, but not considered one of the volunteers developed a middle-ear effusion. In a subsequent study by McBride and colleagues that employed comparable methods and design as described within the beforehand cited study, 32 adult volunteers have been recruited. A related research by Buchman and colleagues evaluated 60 grownup volunteers utilizing a design and strategies just like the earlier two research. Before the nasal problem, three volunteers (5%) had abnormal middle-ear stress, and in two of those topics, a middle-ear effusion developed. None of the topics who had regular middle-ear pressure earlier than the problem developed an effusion, indicating that a rhinovirus an infection may end in a middle-ear effusion if the affected person has a preexisting dysfunction of the tube. These research demonstrated the function that the tube performs in the pathogenesis of middle-ear underpressures, otitis media with effusion, and acute otitis media and are summarized in Table 6�1. Outcomes of an adult volunteer study following intranasal inoculation of influenza A virus demonstrating not solely improvement of abnormal middle-ear pressures and middle-ear effusion but additionally, importantly, an attack of viral and bacterial acute otitis media in one topic. In a highly enlightening study, Buchman and colleagues demonstrated the occasions resulting in the event of not solely otitis media with effusion but, extra importantly, an acute otitis media that developed in a single subject. It is feasible that these microorganisms have been aspirated from the nasopharynx into the middle-ear cavity owing to the excessive unfavorable middle-ear strain. In a newer examine, Doyle and colleagues contaminated 18 adult subjects with influenza A, showing that those individuals who had preexisting good tubal perform decreased the otologic complications of the viral upper respiratory tract an infection. These studies in grownup volunteers had been unique because they demonstrated the relationship of viral upper respiratory tract an infection, middle-ear negative stress, effusion, and acute otitis media. Pathogenesis ninety five Studies of Upper Respiratory Tract Infections in Children An informative scientific investigation by Moody and colleagues additionally demonstrated an identical sequence of occasions in kids, as was documented in grownup volunteers. They reported that when an higher respiratory tract an infection developed within the children, many soon additionally developed middle-ear underpressures, and a few then developed a middle-ear effusion. In a follow-up study, Antonio and colleagues prospectively adopted forty kids of their houses, using daily tympanometry, symptom diaries, and weekly otoscopic examinations, during the respiratory seasons (fall, winter, and early spring) and during times of frequent chilly, which occurred in 22%; 63% of all otitis media episodes occurred throughout an higher respiratory tract an infection. These potential research in youngsters who developed a "wild chilly"-not induced by intranasal inoculation of viruses, as within the adult studies-showed that nearly one-third of episodes of middle-ear effusion occurred prior to the signs and symptoms being obvious. Experiments in Animals In our laboratory over the past forty years, we efficiently produced each underpressures and middle-ear effusion in animal fashions utilizing several methods. In one experiment, excision of a portion of the tensor veli palatini muscle at the pterygoid hamulus within the palate resulted in negative stress within the middle ear followed by an effusion. Complete excision of the tensor tendon resulted in middle-ear underpressures followed by persistent middle-ear effusion. Transection of the muscle resulted in adverse middle-ear stress, or effusion, or both (and in some animals, the center ear returned to normal after the muscle healed). When the tendon was transposed, outcomes had been similar to surgical alteration, however the middle ear quickly returned to regular in a quantity of weeks. Using a noninvasive methodology, Casselbrant and colleagues injected botulinum toxin into the tensor muscle, which resulted in negative stress after which effusion. In these earlier research, middle-ear standing was recognized with otomicroscopy and tympanometry. Animal Models of High Negative Middle-Ear Pressure and Middle-Ear Effusion Outcomes Experiment no 1 2 Reference Cantekin et al. Three methods of surgically altering the tendon of the tensor veli palatini muscle within the monkey that resulted in varying degrees and forms of middle-ear abnormalities, together with development of unfavorable pressure and effusion within the middle ear. As within the earlier study, when the impact of the botulinum toxin resolved, the middle-ear standing returned to regular. Using a special approach, Swarts and colleagues were additionally able to produce unilateral middle-ear effusion in the monkey shortly after inducing middle-ear adverse strain by inflating the middle ear with carbon dioxide. Even although the tube was not altered on this experiment, the research showed the impact of middle-ear adverse pressure in the improvement of middle-ear effusion. All 10 animals within the experiment turned contaminated, and all had tubal dysfunction related to middle-ear underpressures, although no middle-ear effusion developed in any of the ferrets. In an earlier examine by Giebink and colleagues, the nasopharynges of 29 chinchillas have been inoculated with influenza A, which resulted in histopathologic proof of inflammation of the tube and tympanic membrane; middle-ear underpressures had been additionally documented by tympanometry. Outcomes of two studies in monkeys that help the hydrops ex vacuo theory of the pathogenesis of middle-ear effusion. The following describes these scientific sorts and levels of otitis media and relates them to the pathophysiology and pathogenesis related to the tube. Because the tube is obstructed, the middle-ear effusion, owing to the infection, accumulates within the center ear, and the clearance perform of the tube is impaired. For kids with recurrent acute otitis media, an anatomic or physiologic abnormality of the tube appears to be an necessary issue, if not crucial factor.
Buy levaquin 500mg on-lineSegmental areas of sclerosis with broad-based adhesions are an indicator both of sequelae of earlier segmental necrosis and/or crescents medications used to treat adhd discount levaquin 250 mg mastercard. The variety of lesions that may be encountered on this class ranges from diffuse mesangial hypercellularity without necrosis to a severe necrotizing and crescentic glomerulonephritis. About one-quarter of instances exhibit lobular accentuation because of endocapillary hypercellularity with mesangial extension and cellular interposition around the peripheral loops, forming a sample similar to that of different forms of membranoproliferative glomerulonephritis. Multiple immunoglobulins incessantly are encountered and generally are accompanied by proof of the activation of inflammatory mediators, corresponding to a deposition of each classic and alternative complement elements, fibrinogen, and properdin. This sample has been termed a full-house sample of immunoglobulin and complement deposition. These deposits usually are larger and extra ample than in other lessons of lupus nephritis. Mesangial hypercellularity with circumferential mobile interposition is related to the sunshine microscopic pattern of a membranoproliferative glomerulonephritis. This organized look most regularly is seen in the presence of plentiful subendothelial deposits, however it can be current in all classes of lupus nephritis. The crystalline structure is believed by some to represent the presence of cryoglobulins, because comparable buildings are seen in sufferers with idiopathic mixed cryoglobulinemia. There are also numerous mesangial deposits (transmission electron microscopy, �1500). Endothelial cell swelling and proliferation are outstanding, and occasional mitotic figures of glomerular cellular components counsel active proliferation and regeneration secondary to activation of inflammatory cytokines and progress factors. The significance of these constructions is unclear though their presence appears to correlate with illness exercise. A major consequence of severe glomerular irritation with necrosis is the event of both glomerular fibrous crescents and sclerosis, which finally ends up in decreasing glomerular filtration floor and contributes to progressive renal scarring and lack of function. The spikes are outward projections of membrane-like materials between domes that correspond to the subepithelial and intramembranous deposits that are seen on immunofluorescence and electron microscopy. There is diffuse thickening of the peripheral, capillary partitions associated with an increase in mesangial matrix. The pattern is actually identical to that seen in idiopathic membranous nephropathy, besides that mesangial deposits often are present, together with tubuloreticular inclusions. There is diffuse effacement of foot processes in a patient with lupus and nephrotic syndrome. The immediate response of some such sufferers to corticosteroids with remission of proteinuria supports possible minimal change disease�like injury. A typical clinical presentation is heavy proteinuria and renal insufficiency frequently with development to finish stage in the absence of a therapy-induced remission of proteinuria. This collapsing lesion is often focal, and is seen with further underlying focal or diffuse lupus nephritis with typical immune complexes. So-called pauci-immune necrotizing and crescentic glomerulonephritis differs from classical lupus nephritis in that glomerular necrosis and crescent formation are current within the absence of great glomerular immune complex deposits. There is collapse of the glomerular structure with mesangial sclerosis associated with hyperplasia of the visceral epithelium (hematoxylin and eosin, �400). In both situations, treatment options could embody plasmapheresis in addition to immunosuppressive remedy. This is particularly evident in that transformation of renal lesions from one class to one other can happen both spontaneously and on account of remedy. The precise incidence of spontaneous transformation is difficult to decide, however, as relatively few serial biopsy research have been carried out in untreated sufferers. Further, recurrent lupus nephritis in renal transplants could also be of the same, or totally different, class as that seen within the native kidney. A number of studies do recommend that transformation happens commonly and is particularly noted after numerous remedy protocols. Transformation of diffuse proliferative glomerulonephritis to a predominantly membranous nephropathy or a mesangial pattern has been noticed in sufferers present process remission in the course of the course of therapy. These modifications are mirrored in modifications within the demography of age, intercourse distribution, and lupus class of the biopsies of sufferers over the past 10 years at our institution. There was a relative constant increase in age at biopsy throughout this time period suggesting that new therapies could have prolonged life span of sufferers. Immunofluorescence Microscopic Features One issue that has not been given sufficient consideration in the histopathologic analysis of the glomerular lesion of sufferers with lupus nephritis is the function of immunoglobulin isotype and subclass. Most research of the immunofluorescence microscopic findings in lupus nephritis have emphasised the deposition rather than the courses of immunoglobulins discovered. In our own series of sufferers with lupus nephritis, IgG was most frequently current, adopted by IgM and IgA. Less typically, IgE is detected and often is confined to the peripheral capillary wall. This evaluation, however, confirmed a poor correlation between IgG subclass and the severity of the morphologic lesion. Some current reports have advised that IgE deposits in lupus nephritis are related to a poor prognosis. Complement elements, including the membrane attack complicated, fibrinogen, and properdin, often are related to the presence of immunoglobulins, notably within the more extreme lessons of disease. The sample of deposition normally is coarsely granular and corresponds to the dense deposits which are seen on electron microscopy. These further pathologic features embody vascular thrombosis and proliferative and sclerotic vascular lesions, together with inflammatory vasculitis and tubular interstitial lesions. These complicating lesions sometimes are the predominant ones resulting in scientific evidence of renal involvement. In addition, these lesions could turn out to be energetic or progress independently of the primary glomerular lesion. Thus, they should be evaluated independently as additional comorbid elements that may relate to particular further therapeutic maneuvers or that have different prognostic significance. Vascular lesions are frequent and should include intravascular thrombosis, arterial and arteriolosclerosis, and necrotizing vasculitis. A pattern just like that seen in grownup hemolytic uremic syndrome, with a number of capillary and arteriolar thrombi containing fibrin, has been associated with the clinical course of quickly progressive renal failure and is finest recognized as thrombotic microangiopathy. Plasminogen activators are depressed in a few of these sufferers, in whom inhibitors of plasminogen activators are elevated. Because these alterations in plasma ranges of tissue plasminogen activator and 2-antiplasmin could be anticipated to retard fibrinolysis, they had been corrected by administration of the fibrinolytic agent ankyroid to patients with lupus glomerulonephritis. This is associated with the presence of antiphospholipid antibodies or lupus anticoagulant (Jones, �400). Others have confirmed the affiliation of glomerular thrombi with the presence of antiphospholipid antibodies in some, however not all, of those sufferers. Patients with this lupus anticoagulant in their serum are subject to glomerular thrombosis, which may be unbiased of the presence of glomerular inflammation.
Order generic levaquin on-lineFollowing lively dilation symptoms 2 months pregnant purchase levaquin with paypal, the tube passively collapses to return to its resting position starting from the distal end and then to the proximal end, which is important for the muscular clearance perform of the tube (see Clearance). This is as a end result of the center ear and mastoid gas-cell system is a relatively rigid (noncollapsible) fuel pocket surrounded by a mucous membrane by which gases are exchanged between the middle-ear area and the mucosa. Differential strain exceeds 54 mm Hg between the middle-ear house at atmospheric pressure and the microcirculation in the mucous membrane. This represents a diffusion-driven gradient from the middle-ear cavity to the mucosa that may produce an underpressure (relative to ambient pressure) within the middle ear of greater than 600 mm H2O during equilibration. Doyle devised a mathematical mannequin to clarify sure estimates of gas exchanges constants for the center ear. Gas Composition and Pressure in the Nasopharynx, Middle Ear, and Microcirculation of the Middle-Ear Mucosa Compared with Air (mm Hg) Nasopharynx (Mixed Expiratory Air) Lower (566) Low (120) High (27) Higher (47) Middle-Ear Cavity Lower (46) Higher (46) Higher (47) Microcirculation of Middle-Ear Mucosa Lowest (40) Higher (46) Higher (47) 53 and the center ear are equilibrated by the inflow and outflow of gases. Inflow of gas from the nasopharynx into the middle ear is end-expiratory fuel; thus, the pressure regulatory operate of the tube maintains close to equilibrium between exterior and internal pressures, thereby sustaining nearly optimal transducer function of the middle ear and stopping the pathologic consequences that end result from unabated middle ear to mucosa fuel change. Using the microflow approach inside a strain chamber, Elner and colleagues, in a classic study, evaluated 102 adults with intact tympanic membranes and no obvious history of otologic issues (Table 4�3). Patients in group 1 have been in a place to fully equilibrate strain variations across the tympanic membrane. Those in group 2 equilibrated constructive strain, however a small residual adverse strain remained within the middle ear. Subjects in group 3 equilibrated only relative positive stress with a small residual remaining but no unfavorable strain. In an earlier study on the similar laboratory, all 36 "wholesome" ears could equilibrate overand underpressures applied to the ears of adults. During a 4-hour observation interval, the middle-ear strain was approximately normal in alert animals, whereas when the animals were anesthetized and swallowing was absent, the middle-ear strain dropped to 60 mm H2O and remained at that level. The experiment indicated that, normally, middle-ear gases are almost in equilibrium with the mucosal blood tissue gases or inner-ear gasoline pressures. In a later research in the monkey, the rate of constants for the middle-ear cavity to middle-ear mucosa change of oxygen and carbon dioxide is constant with a diffusion-limited course of but not for N2, which indicated a a lot slower price of N2 trade than predicted. These research showed that for relatively short time intervals, middle-ear stress is controlled by experimentally established oxygen and carbon dioxide gradients. In research carried out in our department, apparently healthy adult volunteers were recruited for nasal problem research that concerned virus and allergic antigens. In the first study, we tested six subjects (average age 29 years) who had a adverse otologic history and beforehand regular tympanic membranes till they sustained a traumatic perforation of the tympanic membrane. All were examined utilizing the inflation-deflation and forced-response take a look at of perform, which was thought of regular operate, and were compared with sufferers with otitis media (see Chapter eight,"Diagnosis and Tests of Function"). The remaining eight topics efficiently opened the tube during swallowing when tested by sonometry, equilibrated positive and negative pressure during the inflation-deflation testing, and had normal values for the forced-response testing. Children between 3 and 5 years of age had worse perform than these aged 6 to 8 years. In this research and a subsequent one reported by the identical analysis team, youngsters who had middle-ear negative strain evaluated by tympanometry had poor perform. However, tubal function does enhance with advancing age, in keeping with the reducing incidence of otitis media from infancy to adolescence. High middle-ear pressures have been recognized, by otoscopy and tympanometry, in plenty of youngsters with no apparent middle-ear disease. An inefficient lively opening of the tube in children in all probability explains this frequent finding. Pressure regulation occurs, however solely after the nasopharynx�middle-ear stress gradient reaches a gap strain. Because infants have an inefficient active opening mechanism, they most likely compensate indirectly to regulate strain within the middle ear. One potential compensatory mechanism is crying, and high constructive pressure is obvious when some infants with no middle-ear effusion cry during otoscopy and tympanometry. But in periods of upper respiratory tract infection, nasopharyngeal secretions- and viruses and bacteria-may even be insufflated into the center ear (see Chapter 5, "Pathophysiology"). The mean volume of air passing by way of the tube was found to be reduced by one-third when the body was elevated 20 degrees to the horizontal and by two-thirds when in the horizontal position. The rationalization for this statement stays unclear, nevertheless it could presumably be explained by the relative lack of higher respiratory tract viral an infection affecting the tube through the respiratory seasons of the yr. It has been proven, from adult volunteer nasal virus challenge research, that virus can be recovered from the nose within the absence of the signs and symptoms of a cold. Current thinking is that it either acts as a surge tank of fuel (air) out there to the relatively smaller middle-ear cavity, that the mucosa lining the mastoid gas cells is the primary space for the transfer of gases between the middle ear and mastoid gas cells and the microcirculation, or that each functions coexist. If this considering is correct, then a small mastoid air cell system could be detrimental to the middle ear if the tube is dysfunctional. Likewise, a small mastoid cellular system would enable for a much less efficient gas change between the middle-ear cleft and the microcirculation of the mucosa. In addition, the proximal finish of the system (nasal cavities, palate, and pharynx) should have regular anatomy and physiologic fuel pressures. By distinction, the dye did reflux into the center ear in some sufferers who had middleear illness, especially throughout closed-nose swallowing. This prevents liquid-and abnormal nasopharyngeal sound pressures-from entering the nasopharyngeal finish of the tube. Because the middle ear was intact (neither a tympanic membrane perforation nor a tympanostomy tube was present), the normal structural anatomy of the tube and the middle-ear gas cushion prevented the contrast from getting into the center ear. Submental-vertex spot film taken throughout fluoroscopy, when radiopaque dye was instilled into the nasal cavity of an 8-year-old male who had no historical past or proof of middle-ear disease. The tubal anatomy (the narrowest portion of the tube; the isthmus) and an intact center ear and mastoid prevented reflux of contrast material into the middle ear. In this model, flow would be much less likely as the neck becomes longer and extra likely because the radius of the neck increases (to the fourth power). Naturally, thinner viscosity of liquids would circulate more readily than thicker, and air (gas) would move higher than a liquid. Positive or adverse pressure at either end of the neck (mouth and bulbous parts of the flask) would affect fluid flow in both course. When liquid is instilled into the mouth of the flask (nasopharyngeal) finish of the tube, the liquid stops within the narrow neck (isthmus of the cartilaginous portion of the tube) owing to presents of constructive (back) stress constructed up within the bulbous portion and distal finish of the slender neck of the flask (middle-ear gas cushion). Before describing these two functions, the histology of the mucous membrane of the system needs to be reviewed. The mucous membrane of the middle ear is steady with that of the nasopharynx via the tube and is characterised as respiratory epithelium. This membrane covers all structures throughout the middle ear, including the ossicles, vessels, and nerves. Examination of cells of the mucous membrane throughout the tympanic cavity reveals a gradual change from tall, columnar cells with interspersed goblet cells to shorter, cuboid cells on the posterior portion of the promontory, aditus ad antrum, and mastoid cells. Illustration of the components related to fluid circulate through the neck of the flask mannequin.
Buy discount levaquin 250 mgIn my opinion treatment quadratus lumborum cheap levaquin on line, intranasal oxymetazoline is effective in preventing symptomatic barotrauma during descent in an airplane or throughout scuba diving (see later). When the symptoms are extraordinarily troublesome and intervene with focus, a myringotomy and tympanostomy tube may be required. The symptoms could be intermittent or persistent, and the severity of the complaints could be gentle, moderate, or severe. At the time of the examination, the tympanic membrane may have a normal appearance, and its mobility could or may not be impaired when tested with a pneumatic otoscope or by tympanometry; the tympanic membrane might or will not be retracted. The obstruction of the tube could be anatomic (mechanical), practical (failure of the opening of the tube), or both. Functional obstruction is idiopathic but is as a outcome of of failure of the opening mechanism, which, in flip, could also be attributable to floppy tubal cartilage or abnormalities of the tensor veli palatini muscle or be secondary to the yet to be decided etiology of constriction Role in management of middle-Ear Disease current, there have been essentially no trials of medical remedies for the obstructive type of tubal dysfunction. Even the trials of medical therapies in humans and experiments in animals summarized in Tables 9�1 and 9�2 are disappointing. When nonsurgical strategies are unsuccessful and the signs are troublesome to the patient, then myringotomy and insertion of a tympanostomy tube could also be essential to alleviate the symptoms when the tubes are patent and functioning. This remedy is profitable but is just a "bypass" for the dysfunctional tubal system. The condition, despite the fact that continual, will often resolve with advancing age in children, but some pediatric patients, particularly adolescents, may need to have the tympanostomy tubes changed a number of occasions, and a few could even want a "permanent" tympanostomy tube. This continual disorder can persist all through adult life, for which long-lasting tubes are important. In its excessive kind, the hyperpatent tube is open even at rest (patulous) (see Chapter 5). These last circumstances may be seen when the extracellular fluid is altered by medical treatment of another unrelated condition. Interruption of the innervation of the tensor veli palatini muscle has also been shown to be a cause of a hyperpatent tube. But, when current, this dysfunction could be misdiagnosed as tubal obstruction and inappropriately treated. The affected person frequently complains of listening to his or her personal breathing, voice (autophony), or each within the ear. Patients with chronic tubal obstruction can 171 be "puffers" or use the self-Valsalva maneuver, both of which produce constructive stress within the nasopharynx in an try and equilibrate the negative middle-ear pressure. Otoscopic examination reveals a tympanic membrane that strikes medially on inspiration and laterally on expiration; the motion can be exaggerated with pressured respiration, particularly with one nostril pinched closed. The fluctuation may be exaggerated by asking the affected person to occlude one nostril and shut the mouth during forced inspiration and expiration or by performing the Toynbee or Valsalva maneuver (see Chapter 5 and Chapter 8). If the symptoms are of relatively brief length, the condition could subside without any lively therapy. In youngsters and youngsters, this situation is usually self-limited and doubtless as a end result of age-related changes in the construction and performance of the tube and adjoining areas secondary to speedy development and improvement. Interruption of the neuromuscular component of the tube, similar to from trauma or surgery, may be the trigger, however more generally rapid loss of weight is the underlying pathogenesis. In adults, a neurologic disorder could additionally be present, but in children, the situation is mostly idiopathic. When the symptoms are disturbing and the situation is persistent, energetic therapy is indicated. Myringotomy with insertion of a tympanostomy tube may be helpful in some patients, most likely owing to the coexistence of obstruction and abnormal patency. But tympanostomy tube placement may exaggerate the symptoms if the tube is constantly hyperpatent. I prefer to place a tympanostomy tube previous to a extra aggressive surgical process (described later) because the symptoms might enhance, and a direct measurement of tubal function can be performed to verify the diagnosis (see Chapter 8). Insufflation of powders into the tube and instillation of 2% iodine or 5% trichloroacetic acid solution have also been advocated. They are, for the most part, irreversible and may not enhance the condition or could present solely momentary aid. Stroud and colleagues instructed the transposition of the tensor veli palatini through a palatal incision, however the procedure has not been proven to be safe and effective in a massive number of sufferers by other investigators. Another process reported 2011 placed a curvature inversion plastic tube in 11 sufferers. The middle-ear mucous membrane can actually tear, which may end up in bleeding into the center ear (hemotympanum) secondary to the alterations in middle-ear fuel strain and the pressure within the cabin of the airplane. A middle-ear effusion could be present and is secondary to the unfavorable middle-ear strain. Indeed, Weiss and Frost evaluated 14 children, whose ages ranged from 3 to eleven years and who had middle-ear effusion in one or each ears before an air flight. We advocate an oral decongestant, such as pseudoephedrine hydrochloride, previous to the flight, and a topical nasal decongestant, corresponding to oxymetazoline, instantly before descent; administer two sprays in each nostril and then repeat with two extra sprays in about 5 minutes. Most patients have little or no difficulty during descent with this methodology of prevention. Also, such a person might not develop an acute middle-ear effusion however may have tubal "locking" with excessive middle-ear stress that can be related to acute otologic indicators and symptoms. Evidence that infants have comparatively inefficient lively tubal opening is famous by their crying throughout descent, which most likely inflates their middle ears-a physiologic compensatory mechanism. Keeping potential swimmers, particularly children, out of the water during periods of colds or allergy is one of the best recommendation. The use of an intranasal decongestant spray previous to swimming and diving is an alternate for competitive swimmers, but for the informal swimmer, refraining from this activity is recommended. The pathophysiology throughout descent and ascent is much like that described earlier during flying in an airplane, and the strategies of prevention and treatment are also related. Thus, it would be unwise for a leisure scuba diver who has difficulty equalizing middle-ear pressures throughout scuba training to proceed to pursue this sport. The pathogenesis of this occurring is just like that described earlier throughout air flight and diving. In the human, the allergic condition is extended, which could then lead to an effusion. An animal mannequin that corresponds to the pathogenesis in the human has not been developed. Hurst and Venge and Hurst demonstrated an elevated stage of eosinophil cationic protein in the middle-ear effusion and mucosa of sufferers with allergies and otitis media, which suggests that sort I allergy has a job within the pathogenesis of otitis media. Nevertheless, there does seem to be some proof that chronic and recurrent otitis media with effusion may be related to upper respiratory tract allergy. Therefore, until our data of the origin, technique of diagnosis, and management of allergy in relation to otitis media will increase, when a affected person has recurrent or continual middle-ear illness and proof of higher respiratory tract allergy, management of the allergy ought to be thought of as a therapy option. Because no convincing scientific trials of the treatment options have been reported, nevertheless, no single method of therapy can be beneficial. An allergy workup to identify the offending allergens would be a reasonable possibility, following which allergy control and immunotherapy could be considered. One might argue that the mucosa does produce inflammatory secretions and that clearance is enhanced by the tube.
Generic levaquin 750mg otcFinally medicine in balance buy levaquin 250 mg with mastercard, Chapter 9 offers with the lymphatic vascular system that forms one-way drainage channels transporting tissue interstitial parts again to the venous circulation and passing via lymph nodes. Lymphatic vessels contribute to the regulation of interstitial fluid homeostasis, trafficking of immune cells, and absorption of dietary fats from the gut. The improvement of the lymphatic vasculature, as well as the role of the lymphatic system in pathological situations similar to inflammation and first (genetic origin) and secondary (damaged lymphatic vessels) lymphoedemas, are discussed. Meens Content Introduction seventy three the endothelial organ 73 the endothelial cell surface layer seventy four Heterogeneity of endothelial cells seventy six Functions of the endothelial organ 77 Endothelium-dependent modulation of vascular tone seventy eight Endothelial regulation of blood�tissue exchange 82 Shear stress sensing 85 Conclusion 87 Introduction Endothelial cells make up the monolayer of cells that line blood vessels and act as a physical barrier between circulating blood and vascular easy muscle cells (% Box 6. For a comparatively very long time, endothelial cells had been thought of as little greater than a nucleated protective anti-thrombogenic/anti-adhesive layer. Our appreciation of the metabolic activity of endothelial cells and its central position to the regulation of vascular homeostasis began in 1980 following on from the groundbreaking observations by Furchgott and Zawadzki (1), who initially recognized the function of the endothelium in mediating vascular responses to acetylcholine. It is now generally appreciated that their strategic position determines, to a certain extent, their function, as endothelial cells tightly monitor the transport of plasma molecules, are involved within the regulation of vascular tone, the synthesis and secretion of a big variety of components, and are implicated within the regulation of cell ldl cholesterol, lipid homeostasis, sign transduction, immunity, irritation, and haemostasis. Also, there are clear differences in the circulatory needs of various organs which are reflected within the tightness (junctional properties) of the endothelial cells, as nicely as their interplay with further mural cells. The endothelial organ Endothelial cells could be thought to be a small organ in their very own proper, albeit with a very massive floor space; the estimated whole area of the blood/endothelial interface in people is approximately 7,000 m2. This has been calculated to correspond to a total endothelial mass in the vary of about 1 kg. In addition, endothelial cells could differ when it comes to morphology, mediator launch, antigen presentation, or stress responses. In intact vessels continually exposed to flowing blood, endothelial cells tackle an elongated elliptic kind, orientated in the direction of flow. They are contact-inhibited cells with a very low turnover (estimates of half-life range between 1 and three years). They work together with circulating cells of the immune system and are involved of their activation. Endothelial cells are additionally actively concerned in transporting macromolecules from the vascular lumen into the arterial wall or the extracapillary interstitium. They form connective tissue macromolecules similar to basement membrane proteins, collagen, and proteoglycans. They produce reactive oxygen species, corresponding to superoxide anions, and might thus oxidatively modify low-density lipoproteins during their transit through the endothelium. In some organs, endothelial cells are fenestrated and thus do probably not operate as a permeability barrier. In other organs such as the brain the endothelium has attribute tight junctions and demonstrates solely minimal permeability. Endothelial phenotypes not only differ between species in numerous organs, but also between consecutive vascular sections. For instance, in the kidney the endothelium is fenestrated in peritubular capillaries, discontinuous in glomerular capillaries, and steady in other areas (2). The endothelial cell floor layer the endothelium is incessantly drawn as a thin (cell thickness 0. Although most endothelial cells are very flat (a fact that minimizes diffusional distance), the endothelial cells of venules are tall, plump, and cuboidal (3). The glycocalyx has also been proposed to act as a biomechanical sensor for haemodynamic stimuli such as fluid shear stress (5, 6). Most electron microscopy studies indicate the presence of a glycocalyx with a thickness within the vary of 20 nm. However, this now seems to be an underestimation as fixation methods for electron microscopy are more likely to result in a collapse of gel-like floor constructions with excessive water content (7). More fashionable estimations describe the glycocalyx as being subdivided into bundles with a median thickness of fifty to 300 nm (electron microscopy) and even 2. The construction of the endothelial glycocalyx also appears to differ between fenestrated and continuous endothelium and its thickness and composition varies from organ to organ. Reduced glycocalyx thickness has been described at sites with low and/ or oscillatory shear stress, such as the carotid artery bifurcation, and decreased thickness of the glycocalyx is associated with increased transcapillary transport of lipoproteins (6). Molecular components of the glycocalyx are cell-adhesion molecules concerned in immune reactions and inflammatory processes. Experimental studies recommend that shedding of the glycocalyx happens in inflammation and the lack of the endothelial glycocalyx is associated with elevated E-selectin mediated adhesion of tumour cells to the microvascular endothelial processes that will promote tumour metastasis (10). It is composed of packages resembling densely grown bundles, separated by narrow shiny gaps. Top: pure electron micrograph, Bottom: clarification of endothelium (end, green) and subdivision (red lines) of the endothelial glycocalyx (gly) into packages (arrowheads). Visualization of the glomerular endothelial glycocalyx by electron microscopy using cationic colloidal thorium dioxide. The specific disruption of the glycocalyx, for example, results in thrombin generation and platelet adhesion. Under physiological circumstances, the technology of thrombin is tightly regulated by the inhibitory actions of thrombomodulin, endothelial protein C receptor, and tissue issue pathway inhibitor, all of which are bound to the luminal endothelium. Activation or dysfunction of the endothelium leads to the downregulation of these pure anti-coagulant mechanisms (11).
[newline]Endothelial cells also synthesize and secrete both plasminogen activators (anti-coagulant) and plasminogen activator inhibitors (procoagulant), and the surface layer is the purpose of meeting of parts of the fibrinolytic system, resulting in native stimulation of fibrinolytic exercise. Within 10 to 12 days after intervention the endothelial cells had realigned themselves within the course of blood flow (14). A comparable phenomenon may be noticed in vitro as endothelial cells cultured underneath static situations possess a cobblestone morphology but when uncovered to shear stress for 24 to seventy two hours in addition they slowly develop an elongated and directed morphology. Fenestrated endothelium is present in organs with functions linked to filtration and/or high ranges of transendothelial transport. Most capillary fenestrae possess a skinny 5�6 nm non-membranous diaphragm across their opening that may contribute to selective permeability (15, 16). Mature glomerular endothelial cell fenestrae, nevertheless, lack diaphragms and thus the glycocalyx, which can completely fill and canopy fenestrae in kidney glomerular endothelial cells (8, 9), could contribute to perm selectivity. Discontinuous endothelium is found in sure sinusoidal vascular beds, most notably the spleen and liver. In the latter organ, endothelial cells possess fenestrations of 100�200 nm in diameter that lack a diaphragm and contain gaps (or massive round pores) zero. Interfering with actin polymerization can induce marked and fast adjustments in gap numbers, indicating that the actin cytoskeleton performs a serious role in the regulation of endothelial cell porosity. Moreover, these pores can alter their measurement relying on extracellular calcium concentrations in liver sinusoidal endothelial cells. Heterogeneity of endothelial cells Morphological heterogeneity between capillary endothelial cells Developmentally, endothelial cells arise from the mesoderm by the differentiation of haemangioblasts and/or angioblasts. However, other cell lineages could differentiate into endothelial cells as well, and vice versa endothelial cells might differentiate into different lineages (3). This is probably finest illustrated by the truth that genetic studies aimed toward utilizing particular promoter constructs to label endothelial cells solely handle to affect specific endothelial cell subsets (13).
References - Schessl J, Zou Y, McGrath MJ, et al. Proteomic identification of FHL1 as the protein mutated in human reducing body myopathy. J Clin Invest. 2008;118:904-912.
- Ross MN, Haase GM, Poole MA, et al. Comparison of totally implanted reservoirs with external catheters as venous access devices in pediatric oncology patients. Surg Gynecol Obstet 1988;167(2):141-144.
- Kim YH, Czer LS, Soukiasian HJ, et al. Ischemic mitral regurgitation: revascularization alone versus revascularization and mitral valve repair. Ann Thorac Surg 2005;79(6): 1895-1901.
- Parker LH, Schmidt M, Jin SW, et al: The endothelial-cell-derived secreted factor Egfl7 regulates vascular tube formation, Nature 428(6984):754-758, 2004.
- Meston CM, Frohlich PF: Update on female sexual function, Curr Opin Urol 11:603n609, 2001.
- Ditto PH, Jacobson JA, Smucker WD, Danks JH, Fagerlin A. Context changes choices: a prospective study of the effects of hospitalization on life-sustaining treatment preferences. Med Decis Making. 2006;26(4):313-322.
- Copin MC, Devisme L, Buisine MP, et al. From normal respiratory mucosa to epidermoid carcinoma: expression of human mucin genes. Int J Cancer 2000;86:162-8.
|