|
Professor Mustafa Arici - Professor of Medicine
- Hacettepe University Faculty of Medicine
- Department of Nephrology
- Ankara
- Turkey
Amantadine dosages: 100 mg
Amantadine packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Amantadine 100 mg visaSound waves have compressive and tensile phases the reason above describes the compressive section of a sound wave antiviral eye drops order genuine amantadine online, i. In this case, the neighboring molecules will move to fill the void, leaving a brand new area of rarefraction. This continues one region to the next and the rarefractional disturbance propagates via the medium as a tensile acoustic wave. In most circumstances a tensile wave propagates identical to a compressive wave and with the identical sound speed. This produces alternating compression and rarefraction waves which are referred to as the compressive phase and tensile section of the acoustic wave. For small-amplitude waves (linear acoustics) every level of the waveform strikes on the similar pace, the sound velocity c0. Typically, values for zero and c0 in tissue are 1000 kg/m3 and 1540 m/s, respectively, and so this corresponds to a relative density perturbation of a/ zero = zero. Therefore, the density disturbances related to acoustic waves in medical gadgets, even the very strong waves which are produced in lithotripsy, truly result in very weak (< 5%) compression of the fluid. The relationship between the temporal separation of points on an acoustic wave (t) and the spatial separation of the factors (x) is given by: x = t c 0 (Eq forty nine. For a progressive wave the molecules within the compressed region even have a small web velocity away from the supply. The net velocity of the molecules in a region of area is referred to as the particle velocity (ua) and for a progressive acoustic wave it may be expressed as: u a = pa /0 c zero (Eq 49. For a sinusoidal wave, the spatial extent of one cycle of the wave is called the wavelength. The impression on the density happens as a result of as molecules are compressed collectively, the local density will enhance and in regions of rarefraction the density will lower. The strain in the fluid can equally be written because the sum of two terms: p = p0 + pa (Eq 49. For most fluids, acoustic strain and density are directly associated by an "equation of state" which takes the shape: pa = a c 0 2 (Eq 49. It might be shown beneath that the particle velocity is needed in order to determine the power in an acoustic wave. If the speed is integrated in time, the displacement of tissue may be calculated. It has additionally been suggested that the particle velocity within a biologic goal might produce sufficient strain to damage the cells. Below it will be mentioned how the deformation can even construct up over many pulses and in sure instances may injury tissue. Physically, stress represents a force per unit space and has items of Pascals (Pa). One Pascal is quite a small pressure and atmospheric strain at sea level is roughly one hundred 000 Pa. Power is power per unit time and so the intensity is the energy density divided by the point over which the combination was carried out (Eq 49. It follows that regions of excessive pressure are additionally compressed and have a excessive particle velocity (away from source), and regions of low pressure are rarefied and have a unfavorable particle velocity (towards the source). As the acoustic wave travels, the fluctuations in density, stress, and particle velocity all transfer together. Therefore, in a fluid with recognized materials properties, if one property of an acoustic wave, such as the acoustic stress, is measured, then Eq 49. The quantity of acoustic vitality per unit area is known as the energy flux, power density, energy flux density, or the pulse intensity integral. This is the acoustic equal to the expression from physics "work equals force instances distance," where acoustic pressure is the pressure per unit area and the time integral of the rate offers the distance. Reflection and transmission of sound waves When an acoustic wave encounters a medium with a special impedance, then part of the wave will proceed to propagate in to the model new medium (the transmitted wave) and a half of the wave will be mirrored again in to the original medium (the reflected wave). In terms of acoustic pressure the transmission and reflection coefficients are: Rp = Z2 - Z1 Z2 + Z1 2Z2 Z2 + Z1 (Eq 49. Note that to calculate the integral, the whole stress versus time waveform needs to be precisely measured so that the integration could be done. The vitality E will depend upon both the scale of the realm A and how the intensity varies throughout the area. Indeed, the best acoustic window, which permits the shock wave a pure tissue path to the kidney, is on the flank of the patient (delineated by the ribs, spine. The water�stone transmission is also comparatively high, with 75�95% of the energy being transmitted in to kidney stones. However, a water�air interface has a particularly small coefficient and fewer than 0. This is why shock-wave generators in lithotripsy are water stuffed, why immersion of the affected person in water provides the most environment friendly coupling of shock waves to the physique, and why in dry lithotripters Focusing and diffraction of sound In lithotripsy, focusing of the shock waves is used to focus the acoustic energy on to the stone, whereas lowering the impression on the surrounding tissue as a lot as potential. Lithotripters obtain focusing by varied means, together with using reflectors, acoustic lenses, and spherically curved sources. Regardless of the method used, the physics that describes the focusing of the waves is similar for all these circumstances. An ideal focus could be the case the place all vitality is localized to an infinitesimally small region in space. For a theoretically optimal focusing arrangement, where sound can come in from all angles, diffraction puts a restrict on the size of the focal zone of about one wavelength. For the practical focusing arrangements used in lithotripsy, the place the sound solely comes from one direction, the focal zone may be from a few millimeters to tens of millimeters in dimension. Focal zone the focal zone of a lithotripter (equivalent phrases embrace focal region, sizzling spot, focal spot, focal volume, zone of excessive pressure) of a lithotripter is often ellipsoidal in form with its longest dimension along the axis of the shock wave. The focal volume could be decided by figuring out the zone the place the stress is at least half the maximum stress. Chapter 49 Physics of Shock-Wave Lithotripsy 535 of the focal zone is decided by the diameter of the source, the focal size of the supply, and the frequency content material of the waveform. For a focused acoustic supply that generates a sinusoidal waveform, similar to an ultrasound transducer, there are analytical expressions for the dimensions of the focal zone. The crucial parameters are the wavelength of the sound wave and the half angle of the aperture: flank and the necessity to be in a position to target stones deep in the physique imply that for many lithotripters each the focal length and the diameter of the aperture are round 15 cm. For "weak" shock waves (recall even at the focus of the highest energy lithotripter, the water is compressed by < 5%), the speed of propagation ("part speed") of an acoustic wave is: c phase = c zero + pa /o c 0 (Eq 49. However, the focal area of a lithotripter could be estimated utilizing the formulae for the focal area of a sine wave. Therefore, to make a small focal zone, a shock source with a large diameter aperture and short focal length could be desired. However, the dimensions of the acoustic window in the the place is the coefficient of nonlinearity of the fluid and is a cloth property of the medium. Normally, tissue of more complicated structure has a higher coefficient of nonlinearity. Nonlinearity arises due to two physical processes; first, in areas of excessive strain the local sound speed is elevated above the identical old value, and second the molecules in areas of high stress have the next particle velocity and are convected within the direction of acoustic propagation. The difference between a nonlinear wave and a linear wave is that for a nonlinear wave, totally different elements of the wave journey at totally different speeds, as described by Eq 49.
Purchase amantadine 100mg on lineWith correct tract dilation hiv infection rates california order 100mg amantadine otc, an appropriate size working sheath can then be placed, facilitating the insertion of the endoscopes, working devices, and nephrostomy tube. Use of fascial dilators, Amplatz dilators, metallic coaxial dilators, high-pressure balloon dilators, and radially increasing single-step nephrostomy dilators is well described. In this chapter, the features of each dilation modality and their software shall be reviewed. The introduction of every dilator is normally carried out in a rotational or spinning movement, underneath mandatory fluoroscopic steering. This system is especially useful when faced with the necessity to dilate a closely scarred tract, following earlier percutaneous surgical procedure or within the presence of a retroperitoneal inflammatory course of [2]. The primary drawback of this system is its reliance on the guidewire stability, with potential danger of guidewire kinking resulting in dilation failure. This danger tends to be exaggerated with increased length of tract, similar to in obese patients. Additional theoretical concern is the appliance of excessive guide drive through the tract dilation, resulting in perforation of the medial wall of the renal pelvis, and renal laceration and bleeding [3]. Technique Regardless of the instrumentation utilized in tract dilation, there are several technical steps frequent to every modality. Dilation of the nephrostomy tract follows percutaneous needle puncture in to the calyx of interest. The appropriate placement of the needle is necessary, as the trail of the puncture needle determines which structures are punctured and subsequently dilated. Whenever potential the guidewire ought to be superior in to the bladder � the additional length of guidewire throughout the body reduces the prospect of inadvertent wire displacement and tract loss during subsequent manipulations. The set consists of tapered-tip polyurethane cylindrical dilators, of progressively growing circumference, ranging from 8F to 30F. The primary advantage of this method is conferred by means of a tapered 8F angiographic catheter. The use of the angiographic catheter provides extra stiffening and stability to the guidewire, thereby decreasing the chance of guidewire kinking. The 8F angiographic catheter is inserted over the guidewire beneath fluoroscopic steerage, as an preliminary step. All subsequent larger dilators are inserted over the 8F catheter and guidewire, so as of accelerating diameter. Advancement of each dilator is greatest completed using an alternating clockwise�counterclockwise rotational motion to minimize the probabilities of guidewire kinking. The shoulders of each Amplatz dilator must be superior till totally within the entry calyx. The working sheath is launched final, over the most important Amplatz dilator till the forefront of the sheath overlaps the shoulders of the Amplatz dilator (see Video 20. An additional advantage of this technique is obtainable by the relative rigidity of the dilators, which together with the increased stability and tapered profile, allows higher freedom in dilation of the scarred retroperitoneum. As in the previous system, the primary disadvantage is still the theoretical risk of excessive utility of pressure, leading to renal pelvis perforation and renal parenchymal bleeding [2, 3]. Each dilator is designed to adapt to the lumen of the subsequent successive dilator, starting with an 8F hollow information rod. The preliminary hollow guide rod is superior over a guidewire beneath fluoroscopy, till its tip is positioned inside the renal pelvis. Dilation is achieved with six successive dilators, every increasing in measurement by 4F, finally dilating the tract to either 24F or 26F. A steel guard on the end of each rod represents the endpoint for the insertion of the dilator [4, 5]. The primary advantage of this method lies in its rigidity, which offers assist for dilating through dense scar tissue. This benefit is offset by increased potential for iatrogenic harm, as a end result of difficulty with controlling the strain during dilation. Moreover, the need for handbook stabilization of the central rod throughout the dilation will increase the chance of perforating the renal pelvis. Modification of the usual Alken metal dilators has been described in an try to enhance the protection margin [6]. These modifications have been shown to decrease trauma to the tissues and cut back the prospect of renal pelvis perforation from overadvancing the dilators. Additionally, the nonlocking mechanism allows for elimination of inside dilators, allowing insertion of a ureteroscope and inspection of the tract and collecting system as the tract is being established [6]. Balloon dilator systems the use of balloon dilators was pioneered within the subject of interventional angiography and has subsequently been tailored for use in other disciplines. The application of balloon dilation to percutaneous renal surgical procedure has been a major advancement. Percutaneous nephrostomy tract balloon dilators are meant for creation of tracts in a rapid, single step, eliminating the need for serial dilation. They are designed to be launched in to the accumulating system over a guidewire and tract dilation is carried out under fluoroscopic steerage. Pressures of up to 20 atm could be easily achieved with this method, although in general, a lot decrease pressures are normally sufficient for tract creation. Balloon inflation permits for full expansion of the balloon, which is followed by insertion of a working sheath over the balloon, in a rotational method. The major advantage of the balloon dilation know-how lies in the reality that the tract is created utilizing lateral, somewhat than angular, shearing forces. In principle, lateral forces are less traumatic and reduce the possibility of large vessel damage and resultant hemorrhage. An further advantage is the elimination of serial dilation, which saves operating room time [7]. The dilation can also be more managed, as the balloon can simply be stabilized during Chapter 20 Dilation of the Nephrostomy Tract 235 the inflation. In earlier expertise, the usage of balloon dilators was discovered to result in a lower price of blood transfusions in comparison to Amplatz and fascial dilators [8, 9]. Contemporary series comparing the Amplatz and balloon dilation systems have instructed the differences in issues may not be vital [10, 11]. The main drawback of balloon dilators are their relative larger price in comparison with the opposite techniques. In a case where more than one tract is required, the same balloon can be used once more. Other concerns with the balloon catheters include an incapability once in a while to dilate through dense scar tissue and the risk of balloon rupture inflicting barotrauma. In most conditions, the balloon dilator is superior until the proximal radio-opaque marker is positioned inside the entry calyx (see Video 20. Correct placement of the balloon dilator is important to present a helpful tract and to keep away from vital bleeding.
Cheap 100mg amantadine free shippingIntrarenal Bacillus Calmette-Guerin remedy for higher urinary tract carcinoma in situ how hiv infection occurs buy amantadine with a visa. Complications of intracavitary Bacillus Calmette-Guerin after percutaneous resection of higher tract transitional cell carcinoma. Technique of mitomycin C instillation in the remedy of upper urinary tract urothelial tumors. Adjuvant mitomycin C following endoscopic remedy of higher tract transitional cell carcinoma. Setting a new standard for topical therapy of higher tract transitional cell carci- 102. This condition may be congenital or acquired, the congenital kind being the more widespread. The creation of smaller-caliber endoscopes [2], and improvement of laparoscopic reconstructive strategies, laser expertise, and robotics have diversified the therapy options for this condition. Although the efficacy, and decreased morbidity, hospital keep, and wish for analgesia with endopyelotomy have been clearly demonstrated, several issues have still not been utterly resolved. In the period of minimally invasive laparoscopy and robotic-assisted surgical procedure, is there nonetheless a role for endopyelotomy Open surgical correction was the only mode of therapy for this condition before the introduction of endoscopic and laparoscopic strategies, and has been considered the gold normal of treatment for this condition, with success charges over 90% [3]. As compared with different remedy options, ureteroscopic retrograde endopyelotomy is much less invasive, requires less operating room time, allows the procedure to be carried out on an outpatient foundation or with a very short hospital stay, and is related to a shorter convalescence interval [1, thirteen, 25�29]. Also, the preliminary report of ureteral stricture formation due to thermal damage from transmission of the electrocautery present has been eliminated with using insulated ureteroresectoscopes and holmium laser fibers [30]. Among absolutely the contraindications are patients with lively an infection and bleeding diathesis. Patients with a comparatively long size of obstruction, normally higher than 2 cm, are greatest managed either with open surgical, laparoscopic, or roboticassisted techniques. Patients with ipsilateral differential renal perform of lower than 20% and severely decreased parenchymal thickness could be given a trial of drainage and re-evaluation [15] or ought to be provided a laparoscopic simple nephrectomy for a poorly functioning or nonfunctioning kidney. Patients with huge hydronephrosis ought to be treated with dismembered pyeloplasty, both open surgical, laparoscopic, or robot assisted, because of the need for trimming and discount of the redundant renal pelvis. A single-setting, onestage procedure was subsequently described by Soroush and Bagley in 1998 [11]. However, many establishments now think about endopyelotomy a possible first-line therapy possibility for the therapy of this condition [13�16]. Currently, a retrograde endopyelotomy could be carried out in three ways: (1) utilizing a rigid ureteroscope and a cold-knife, electrocautery, or holmium laser incision; (2) utilizing a flexible ureteroscope and electrocautery or laser incision; and (3) in rare select cases, utilizing a balloon with a chopping wire (Acucise) [15]. Additionally, an rising strategy of dilation and cold-cut incision with a peripheral chopping balloon, which was initially designed for angioplasty, is presently being investigated [17�19]. Although once thought-about a contraindication due to poor outcomes, revealed collection report that the type of ureteral insertion has no important influence on the outcome of endopyelotomy [24], and that patients with crossing vessels had long-term success with retrograde endopyelotomy [14]. Lastly, patients with identified intractable stent intolerance ought to be considered candidates either for an antegrade endopyelotomy or an open pyeloplasty with a nephrostomy tube, and never for ureteroscopic endopyelotomy. Above all, preoperative placement of the stent allows analysis of any degree of stent intolerance and identifies improvement of renal function after drainage. A B Step-by-step operative technique the required instrumentation is listed in Table 42. After either a general or a spinal anesthesia, the patient is placed within the lithotomy position. Caution is taken so that every one stress factors are well cushioned, and antiembolic stockings are used in high-risk sufferers. A retrograde pyelogram can assess any resolution of hydronephrosis and can be utilized as a prognostic indicator. The next step varies depending on whether or not the endopyelotomy is finished with electrocautery by way of a ureteroresectoscope or whether or not a holmium laser is used by way of a rigid, semi-rigid, or flexible ureteroscope. A balloon dilator may be passed over the guidewire and the ureteral orifice dilated in case of issue advancing the ureteroscope throughout the ureter. If necessary, one other guidewire could be passed by way of the ureteroscope and the slender area subsequently balloon dilated. A 365-m holmium laser fiber, when using a inflexible or semi-rigid ureteroscope, or a 200-m fiber in the case of a flexible ureteroscope, is passed by way of the working channel of the ureteroscope. After hemostasis of any venous bleeding is carried out, the laser fiber and ureteroscope are removed. An endopyelotomy stent is positioned under fluoroscopic management, leaving Ureteroscopic endopyelotomy with electrocautery A 5F open-ended catheter is handed over the super-stiff wire. Short and shallow strokes must be performed and aggressive and deep incisions prevented. The incision is carried down until periureteral fats is seen and the ureteroresectoscope enters the renal pelvis with ease. Postoperative care the vast majority of patients are discharged either the same day or inside the first 24 h following the process. Oral antibiotics, usually quinolones, are given for 3�5 days; oral antispasmodics and/or oral anticholinergics are given as wanted in case of irritative bladder symptoms. Patients are followed-up with renal ultrasound or renal scan every 4�6 months during the first yr and yearly thereafter or as needed. Success following endopyelotomy is measured by evaluating enchancment of the function and drainage of the concerned kidney and alleviation of symptoms. Also, the open-ended catheter could serve to constantly drain the renal pelvis of the irrigant used in the course of the process, as soon as the wire is removed. The ureteroresectoscope is passed immediately alongside the insulated guidewire with the cold knife in place. The electrocautery component is true angled and would impede imaginative and prescient if positioned during the insertion of the ureteroresectoscope [1]. If necessary, another guidewire could be handed through the self-dilating ureteroscope and the narrow space is balloon dilated. These sufferers included seven pediatric sufferers, 4 solitary kidneys, two horseshoe kidneys, and one ptotic kidney. Seventy-nine p.c of the patients had been discharged house on the identical day, and 97% of them within 24 h. Of the 139 sufferers 32 (23%) required subsequent procedures to deal with recurrence of obstruction, displaying an overall long-term success fee for retrograde ureteroscopic endopyelotomy of 77%. Significant bleeding requiring emergent nephrectomy is one other possible complication that justifies the need for vascular or three-dimensional (3D) radiographic studies to identify aberrant vessels. Minor problems of retrograde ureteroscopic endopyelotomy embody proximal stent migration, stent intolerance, minor bleeding, and urinary tract infection after manipulation. Most of those issues are alleviated after elimination of indwelling ureteral stents. The routine use of antispasmodic and anesthetic medicine after surgical procedure improves tolerance to the stent and decreases complaints from the patient.
Generic amantadine 100 mg visaUntreated or uncared for candidiasis might progress to fungal balls or abscess formation antiviral brand order amantadine 100 mg otc. Sonography is commonly used because the initial imaging procedure however retrograde and antegrade pyelographies are used for biopsy, analysis, and remedy [149]. The benefits Fluconazole has been reported as an efficient antifungal bladder irrigant [132]. Percutaneous fluconazole irrigation was efficiently used to treat candidiasis in nephrostomy tubes that was unresponsive to systemic intravenous remedy [126]. Fluconazole solution was used as an antifungal irrigant in 20 patients with a nephrostomy tube or suprapubic catheter who introduced with two constructive urine cultures for Candida. In 17 (85%) sufferers, Candida was eradicated from the urine by the third to sixth day of irrigation. Amphotericin B Amphotericin B was first isolated as a by-product ensuing from the fermentation means of Streptomyces nodosus and is a member of the polyene macrolide class of antibiotics [134]. Depending on the drug focus and susceptibility of the organism, amphotericin B may be either fungistatic or fungicidal. Oxidation-dependent amphotericin B-induced stimulation of macrophages of the host cells additionally might contribute to its antifungal properties [135]. Amphotericin B deoxycholate has been used in the therapy of most fungal infections, with nephrotoxicity being the most typical severe persistent antagonistic effect[136]. Fortunately, this azotemia is usually reversible and sodium loading with intravenous saline and hydration might stop or scale back the severity of the nephrotoxicity. In an effort to cut back systemic unwanted aspect effects, new formulations of amphotericin B have been developed. These encapsulate amphotericin B in lipid vehicles that are taken up by the reticuloendothelial system concentrated in liposomes. Monocytes/macrophages within the peripheral blood are thought to take up the drugladen liposomes and move them to the location of an infection, where free active drug is thought to be launched via the motion of phospholipases [127]. Bladder irrigation with amphotericin B is extensively used and has become a regular treatment, though it has not undergone managed trials [134, 137�141]. Streptokinase has additionally been used in conjunction with amphotericin B within the therapy of pyonephrosis. This was profitable in clearing the fungal balls, relieving obstruction, and rendering the urine sterile, and highlights the potential position for streptokinase in cases of renal candidiasis refractory to current treatment protocols. The role of antifungal agents for upper tract fungal infections will require ongoing investigation. In circumstances of pyonephrosis probably the most reported approaches would include placement of a nephrostomy tube and local instillation of an antifungal agent such as amphotericin B. The benefit of topical intracavitary remedy is that extremely poisonous medicines can be delivered to the positioning of infection quite than systemically, which can decrease potential unwanted effects. Percutaneous instillation of topical antifungal agents corresponding to amphoteracin B permits administration of highly toxic antifungal medicine to sufferers with localized infection, thereby minimizing systemic unwanted side effects. Cystine nephrolithiasis: report of case with roentgenographic demonstration of disintegration of stone by alkalinization. Limitations of caspofungin within the treatment of obstructive pyonephrosis because of Candida glabrata infection. Intermittent irrigation system for dissolution of renal calculi monitored by laptop. Expedited struvitestone dissolution utilizing a high-flow low-pressure irrigation system. Conclusions Percutaneous remedy delivers drugs or chemotherapeutics instantly in to the amassing system and could be extremely effective at targeting the pathology. Direst remedy permits excessive native concentrations to be delivered while avoiding potential systemic problems. Stone dissolution through chemolysis stays an choice for urologists even within the introduction of more refined modalities within the treatment of urolithiasis. Intracavitary immunotherapy/chemotherapy is a useful adjuvant therapy publish endoscopic management 306 Section 2 Percutaneous Renal Surgery: Other Uses of Nephrostomy Access 38. Reduced glomerular filtration fee and hypercalciuria in major struvite nephrolithiasis. A randomized double-blind trial of Lithostat (acetohydroxamic acid) in the palliative remedy of infection-induced urinary calculi. A randomized double blind examine of acetohydroxamic acid in struvite nephrolithiasis. Properties of organic acid solutions which determine their irritability to the bladder mucous membrane and the impact of magnesium ions in overcoming this irritability. Dissolution of phosphatic urinary calculi by the retrograde introduction of a citrate resolution containing magnesium. Combination of chemolysis and shock wave lithotripsy in the remedy of cystine calculi. Complex struvite calculi treated by primary extracorporeal shock wave lithotripsy and chemolysis with hemiacidrin irrigation. Crystalline composition of urinary stones in recurrent stone formers: quantitative observations on the crystalline composition of urinary stones. Urothelial harm to the rabbit bladder from alkaline irrigants useful within the remedy of uric acid stone. Treatment of cystine stones: mixed approach utilizing open pyelolithotomy, percutaneous pyelolithotripsy, extracorporeal shock wave lithotripsy and chemolysis. Chapter 26 Percutaneous Instillation of Chemolytic, Chemotherapeutic, and Antifungal Agents 60. Chemolysis of struvite stones by acidification of synthetic urine � an in vitro study. Dissolution of urinary stones by calcium- chelating brokers: a study using a model system. Urothelial harm from ethylenediaminetetraacetic acid used as an irrigant in the urinary tract. Long-term expertise with Bacillus Calmette-Guerin remedy of upper urinary tract transitional cell carcinoma in sufferers not eligible for surgical procedure. Percutaneous bacillus calmette-guerin perfusion of the higher urinary tract for carcinoma in situ. Durable response of a carcinoma in situ of renal pelvis to topical Bacillus Calmette-guerin. Instillation of Bacillus Calmette-guerin in to the renal pelvis of a solitary kidney for the therapy of transitional cell carcinoma. Management of stage T1 superficial bladder cancer with intravesical bacillus Calmette-Guerin remedy. Long-term follow up of sufferers treated with 1 or 2, 6-week courses of intravesical bacillus Calmette-Guerin: evaluation of attainable predictors of response freed from tumor. Recurrence, development and success in stage Ta grade three bladder tumors handled with low dose bacillus Calmette-Guerin instillations. Has a 3-fold decreased dose of bacillus CalmetteGuerin the same efficacy against recurrences and development of T1G3 and this bladder tumors than the standard dose Percutaneous management of transitional cell carcinoma of the renal collecting system: 9-year experience. Bacillus CalmetteGuerin perfusion therapy for carcinoma in situ of the upper urinary tract.
100mg amantadine overnight deliveryOverview � In the human circulatory system how hiv infection occurs amantadine 100mg low price, three primary pathophysiologic processes may cause circulatory insufficiency, or shock (Tables 4-4 and 4-5). Distributive shock � In distributive forms of shock, widespread vasodilation decreases the peripheral resistance considerably, thereby reducing the blood pressure to insufficient levels. Septic shock: cytokines released in response to toxins trigger widespread vasodilation (called "heat" shock) c. Conducting airways: " resistance as a result of organized in collection Bronchi comprise supportive cartilage rings that forestall airway collapse during expiration. These include the nostril, mouth, pharynx, larynx, trachea, bronchi, and conducting bronchioles. Clinical observe: In bronchial asthma, the smooth muscle of the medium-sized bronchi becomes hypersensitive to certain stimuli. This airway narrowing produces turbulent airflow, which is usually appreciated on examination as expiratory wheezing. Cystic fibrosis and ventilation-associated pneumonia are other examples of situations associated with dysfunction of the mucociliary tract. These embody respiratory bronchioles, alveolar ducts, and alveoli, the place gas exchange happens. Despite their smaller measurement, airway resistance is less than in conducting airways, as a result of the respiratory airways are arranged in parallel, and airflow resistances in parallel are added reciprocally. This is a skinny barrier that separates the alveolar air from the pulmonary capillary blood, through which fuel change must happen. Type 2 epithelial cells are a lot less quite a few but are essential in producing surfactant (stored in lamellar bodies). When the pulmonary membrane has been damaged, sort 2 epithelial cells are in a position to differentiate in to kind 1 epithelial cells and impact restore of the pulmonary membrane. Diaphragm: most essential muscle of respiration Accessory muscles: sternocleidomastoid, scalenes, pectoralis major; important in forceful respiratory B. This enlargement happens primarily on account of diaphragmatic contraction and, to a lesser extent, contraction of the external intercostal muscular tissues. In patients with respiratory misery, the abdomen may very well be "sucked in" while the accessory muscle tissue of inspiration are contracting. This is named paradoxical respiration and is an indicator of impending respiratory failure. Driving force for inspiration � A negative intrapleural stress is created by movement of the diaphragm downward and the chest wall outward. The distinction between pleural and alveolar pressures is referred to because the transpulmonary stress. Note that alveolar strain equals zero at the end of a tidal Tissue resistance: friction generated by pleural surfaces sliding over each other throughout inspiration Expiration during normal breathing: passive course of because of elastic recoil of lungs and chest wall Expiration during exercise or in lung disease: lively course of requiring use of accent muscle tissue " Intrapleural pressure: caused by movement of diaphragm upward and chest wall inward Airflow resistance throughout expiration: primarily due to # airway diameter from " intrathoracic pressures � Tissue resistance: friction that happens when the pleural surfaces glide over each other as the lungs inflate C. Overview � Usually a passive course of by which leisure of the diaphragm, mixed with elastic recoil of the lungs and chest wall, forces air from the lungs � During forceful breathing. Contraction of those muscle tissue helps to depress the rib cage, which compresses the lungs and forces air from the respiratory tree. Driving forces for expiration � An improve in intrapleural pressure is created by motion of the diaphragm upward and the chest wall inward. Additionally, the recoil forces from the alveoli that have been stretched throughout inspiration promote expiration. Clinical notice: If the lung were a simple pump, its maximum attainable transport of gas out and in would be restricted by exhalation. During expiration, the last two thirds of the expired very important capability is largely unbiased of effort. The discount in small airway diameter with resultant increase in airway resistance is the most important determinant of this phenomenon. In contrast, giant airways are largely spared from collapse by the presence of cartilage. In the lung, air viscosity and airway length are basically unchanging constants, whereas airway radius can change dramatically. For instance, airway diameters are decreased by clean muscle contraction and extra secretions in obstructive airway illnesses corresponding to asthma and persistent bronchitis. Although that is true for the smaller airways, during which the whole cross-sectional area is massive and the airflow velocity is gradual, airflow in the higher airways is often turbulent, as evidenced by the bronchial sounds heard during auscultation. Under regular situations, many of the complete airway resistance truly comes from the large conducting airways. By distinction, the small airways (terminal bronchioles, respiratory bronchioles, and alveolar ducts) provide comparatively little resistance. Most different lessons work by preventing bronchoconstriction or by inhibiting inflammation (which reduces airway diameter); these include steroids, mast cell stabilizers, anticholinergics, leukotrienereceptor antagonists, and lipoxygenase inhibitors. Large airways: contribute most to airway resistance; organized in collection with small total cross-sectional area Small airways present relatively little resistance: organized in parallel; large whole cross-sectional space; slow/laminar move Compliance work: work required to overcome elastic recoil of lungs; largest element of labor of breathing three. Compliance resistance (work) � As the lungs inflate, work should be performed to overcome the intrinsic elastic recoil of the lungs. Change in lung volume (mL) Compliance resistance work Tissue resistance work Airway resistance work 500 250 Inspiratory curve �1 �2 Change in pleural strain (cm H2O) 5-5: Relative contributions of the three resistances to the whole work of respiration. Pathology notice: In emphysema, destruction of lung parenchyma leads to elevated compliance and a decreased elastic recoil of the lungs due to destruction of elastic tissue by neutrophil-derived elastases. During inspiration, maximal compliance occurs in the midportion of the inspiratory curve. The distinction between the inspiration curve and the expiration curve is referred to as hysteresis. Note that the saline-inflated lungs are more compliant than air-filled lungs owing to the reduction in floor pressure, which reduces the collapsing strain of alveoli. Note the orientation of the hydrophilic "head" within the alveolar fluid Clinical observe: the collapse of many alveoli in the same area of lung parenchyma results in atelectasis. Surfactant is a posh phospholipid secreted on to the alveolar membrane by type 2 epithelial cells. There is due to this fact a high danger for respiratory failure and neonatal respiratory misery syndrome (hyaline membrane disease) in these infants. The price of diffusion is dependent on the partial strain (tension) of the gases on either facet of the membrane and the surface space available for diffusion, amongst different components. Example: Assume a mountain climber at high altitude is exposed to an atmospheric strain of 460 mm Hg. This is the amount of gas that may diffuse across the pulmonary membrane in 1 minute when the strain difference throughout the membrane is 1 mm Hg. In varied forms of lung illness, the diffusing capability could also be lowered to such an extent that O2 trade becomes diffusion restricted. Perfusion-limited exchange � Gas equilibrates early along the size of the pulmonary capillary such that the partial pressure of the gas in the pulmonary capillary equals that within the alveolar air. Pressures in the Pulmonary Circulation � Despite receiving the whole cardiac output, pressures in the pulmonary circulation are remarkably low compared with the systemic circulation.
Buy amantadine 100mg amexThe equipment required is the hemodialysis machine anti bullying viral video buy discount amantadine on line, pediatric dialyzer with tubings and dialysate fluid. Vascular entry is critical for removing and returning giant portions of blood required for the process. This is normally achieved utilizing a double lumen catheter inserted in to the internal jugular, femoral vein or subclavian vein. Most kids are maintained on a hemo dialysis regimen of 3-4 hr, 3 times every week. The contrasting char acteristics of acute kidney harm in developed and developing coun tries. Continuous hemofiltration offers smoother management of ultrafiltered quantity and gradual correction of metabolic abnormalities in unstable sufferers. These therapies are helpful when large amount of fluids have to be eliminated in sick and unstable sufferers. If interstitial nephritis is suspected, the offending agent should be withdrawn and oral corticosteroids given. The outlook is satisfactory in acute tubular necrosis with out complicating factors. Other factors related to poor consequence embrace delayed referral, presence of complicating infections and cardiac, hepatic or respiratory failure. Maintenance of diet and prevention of infections is extremely crucial in bettering outcome. Renal failure could occasionally be the first manifestation of a congenital anomaly of the urinary tract. Symptoms of renal failure could additionally be insidious, together with lethargy, puffiness and some decline in urine output. Renal vein thormobosis is suspected in at-risk neonates with hematuria, enlarging flank mass, thrombocytopenia and azotemia. Features suggestive of urinary tract obstruction embody an stomach mass, hypertension and oligoanuria. Serum creatinine ranges are excessive at birth (reflecting maternal levels) and decrease to below zero. Failure of discount or rise of serum creatinine indicates impaired renal perform. Sudden distention of peritoneal cavity might trigger respiratory embarrassment or apnea. Since chiefly shigatoxins 1 and a couple of are implicated, the sickness is also known as shigatoxin E. The microangiopathic lesions chiefly affect interlobular arteries and end in extreme hypertension and progressive renal insufficiency. Defective cobalamin metabolism results in a extreme form presenting in early infancy. Following a prodrome of acute diarrhea or dysentery, patients present sudden onset of pallor and oliguria. The capillary lumen is narrowed by swollen endothelial cells, blood cells and fibrin thrombi. A number of medication are dialyzable and appropriate quantities should be added to complement for their losses. The consequence is said to the underlying condition until the renal failure is prolonged beyond a number of days. They are characterised by microangiopathic hemolytic anemia, thrombocytopenia and acute renal insufficiency. Cytotoxin mediated harm to endothelium in the renal microvasculature results in localized coagulation and fibrin deposition. A classification of hemolytic uremic syndrome and thrombotic thrombocytopenic purpura and related problems. Peritoneal or hemodialysis could additionally be essential to prevent compli cations of renal insufficiency. Plasma exchanges are initiated as early as potential, performed daily until hematological remission, and then much less regularly. Patients with anti-factor H antibodies benefit from immunosuppression with brokers that reduce antibody manufacturing. Factors suggestive of poor end result embody oligoanuria for greater than 2 weeks, extreme neurological involvement and presence of cortical necrosis. At the preliminary levels, management aims at maintaining nutrition and retarding progression of the renal failure. Later, therapy of issues and renal substitute therapy within the form of dialysis or transplantation is required. Loss of urinary concentrating capability results in frequent passage of urine, nocturia and elevated thirst. Resistance to the motion of development hormone, the levels of that are elevated, is taken into account to be liable for progress failure. Abnormalities in metabolism of calcium and phosphate and bone disease results from hyperphosphatemia, lack of renal formation of 1, 25-dihydroxyvitamin 03, deficiency of calcium, continual acidosis and secondary hyperparathyroidism. The blood strain could additionally be increased and optic fundi show hypertensive retinopathy. Severe proximal muscle weak point, peripheral neuropathy, itching, purpura and pericarditis are late options. Investigations Treatment of Reversible Renal Dysfunction Common conditions with potentially recoverable kidney perform embody an obstruction in the drainage, recurrent urinary tract infections with vesicoureteric reflux and decreased renal perfusion as a outcome of renal arterial stenosis. Retarding Progression of Renal Failure Hypertension and proteinuria lead to elevated intra glomerular perfusion, adaptive hyperfiltration and pro gressive renal damage. Longterm therapy with angiotensin changing enzyme inhibitors has been proven to reduce proteinuria and will retard progression of renal failure. The patient ought to be investigated to discover the cause of renal failure and detect reversible factors. Blood counts and ranges of urea, creatinine, electrolytes, pH, bicarbonate, calcium, phosphate, alkaline phos phatase, parathormone, protein and albumin are obtained. Blood levels of ferritin and transferrin saturation are obtained in patients with anemia. A food regimen high in polyunsaturated fat, similar to corn oil and medium chain triglycerides and complex carbohydrates is preferred. Excessive use of diuretics, overzealous restriction of salt and gastroenteritis might lead to dehydration that should be corrected. Blood must be transfused slowly, since it might irritate hypertension and coronary heart failure. Urinary tract and other infections must be promptly handled with effective and least poisonous drugs. Optimization of caloric and protein intake and treatment of mineral bone disease is necessary. Administration of recombinant human growth hormone improves growth velocity in youngsters with continual renal failure.
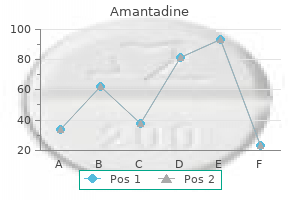
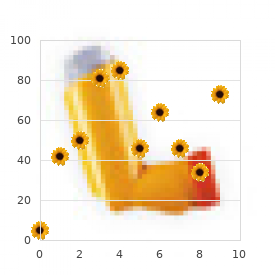
Buy cheap amantadine 100mg lineNote that the bubble continues to develop long after the shock wave has handed (5 s time frame) hiv infection on tongue generic 100 mg amantadine with visa, Chapter 49 Physics of Shock-Wave Lithotripsy 539 referred to as inertial cavitation, as the dynamics of the bubble are no longer driven by acoustics however as an alternative by the inertia of the fluid surrounding the bubble. While the bubble is giant, some amount of gas and vapor from the fluid will diffuse in to the bubble. The bubble will then collapse by virtue of the near vacuum contained in the bubble and the roughly 1 atm of ambient pressure within the surrounding fluid. The collapse may be very violent and the fuel that diffused inside is heated and compressed to such an extent that it could produce light [48]. The major collapse is followed by rebounds after which the gasoline that had diffused in to the bubble will slowly diffuse back out in to the fluid. This distinctive "doublebang" signature can be utilized to detect the cavitation occasions [48]. For a spherical bubble, the amplitude of the scattered gentle varies in a known method because the bubble radius adjustments. This technique is prepared to capture most of the temporal and spatial scales related to the dynamics of a lithotripsy-excited cavitation bubble. This means the method will solely yield qualitative information about bubble clouds or nonspherical bubbles, each of that are quite common in lithotripsy-induced cavitation. Acoustic detection in vivo Acoustic detection of bubbles is very powerful, in part as a result of it may be used to characterize bubble dynamics inside dwelling subjects. The timing and amplitude of the 2 emissions is influenced by numerous factors similar to the dimensions of the preliminary bubble and the amplitude of the lithotripter pulse. Measuring cavitation There are numerous strategies by which cavitation can be measured: High-speed pictures Bubble conduct can be observed using a high-speed camera in an in vitro setting [49-52]. During the expansion part the bubble needs to be imaged at millimeter length scales and tens of microsecond time scales. At the nadir of the collapse, the bubble radius is less than 1 m and the dynamics of the collapse is at nanosecond time scales. The remnant bubble left after the rebounds is of the order of 10 m and slowly dissolves over tons of of milliseconds. Thus, the range of temporal and spatial scales makes it nearly inconceivable to seize all of the bubble dynamics photographically. Laser scattering of single bubbles the dynamics of a single spherical bubble can be measured very exactly by laser scattering [53]. Two targeted transducers are placed in order that their ellipsoidal focal zones intersect. Acoustic emissions that happen in the shaded area of intersection may be localized by trying to find simultaneous events on both transducers. It has been noticed that cavitation leads to pitting on metal foils and the quantity and depth of pits can be used to assess the violence of cavitation [38, 59, 60]. An electromagnetic probe gadget has been used to measure the mechanical force exerted on a metal ball by both the incident shock wave and the cavitation exercise [61]. The excessive pressures and temperatures in the inside of the bubble provide an environment which can produce gentle emissions (sonoluminescence) and also end in enhanced chemical reaction charges (sonochemistry). Production of sunshine and by-products from chemical reactions have each been used to quantify cavitation exercise [53, 58]. These are secondary measurements of the cavitation area and interpreting the results when it comes to bodily processes may be sophisticated. F1 Spark Plug Brass Ellipsoidal Reflector 2 cm Physics of medical lithotripsy Shock era and focusing Three shock-wave generating rules have been utilized in scientific lithotripters. Misalignment by only a few millimeters can result in a big loss in focusing, and a lengthening and broadening of the focal zone. Therefore, from shot-to-shot there can be significant variation (upwards of 50%) within the amplitude of the shock wave and there could be some shift within the place of the focal zone at the target. However, it has been proven that this direct wave can affect the cavitation generated by the centered wave [62]. Some lithotripter manufacturers have found methods to improve the lifetime of their electrodes, such as by encapsulating them and filling the casing with an applicable electrolyte [63]. When the coil is happy by a short electrical pulse, the plate experiences a repulsive pressure and that is used to generate an acoustic wave. In both instances, focusing could be very reproducible and variation in measured stress waves is less than 10%. The amplitude of the wave at clinically related power settings is often high sufficient that nonlinear distortion happens during propagation, and a shock is produced before the wave reaches the major focus. This peak likely has little impression on the stress inside the stone but might have an effect on the cavitation dynamics. When a voltage is utilized to a piezoelectric crystal, it deforms and creates an acoustic wave. This focus is very reproducible and very small variations in the focal waveforms are reported. Coupling of the shock source to the body Efficient switch of acoustic energy from one medium to one other solely happens when the acoustic impedances 542 Section 4 Shock-Wave Lithotripsy lithotripter. All lithotripters have a focus, however lithotripters differ within the dimensions of the zone of excessive stress (focal zone) that surrounds this level. The dimensions and the stress characteristics of the focal zone are the most important features that distinguish one lithotripter from one other. There are many definitions of the focal zone that may be appropriate for lithotripsy. The maximum peak positive pressure is the highest worth of p+ within the field of the lithotripter and the situation of the utmost peak optimistic strain is defined as the focus [20]. The ensuing focal zone is normally an elongated, elliptical, "cigar-shaped" quantity. Because completely different lithotripters, even the identical sort of lithotripter, could perform somewhat differently, and since investigators have used different means to map the acoustic subject of their lithotripters, revealed values for peak pressures and dimensions of the focal zone of a given kind of lithotripter could not coincide perfectly. The half-maximum focal zone (also generally known as -6 dB focal zone as the contour corresponds to the strain being 6 dB less than on the maximum) is recommended are very shut. A water�tissue interface results in superb coupling and theoretically it must be potential to transfer greater than 99% of the power of the shock wave in to the body. This is ideal besides that bubbles that drift up from the spark hole or the cavitation bubbles that form along the path of the shock wave, have the potential to gather towards the pores and skin of the affected person and interfere with the propagation of subsequent shock waves. Dry lithotripters Most present lithotripters have the shock-wave source mounted in a "remedy head" which is full of water. The remedy head is capped by a skinny rubber membrane, which is pressed towards the affected person and thru which the shock wave passes. The water within the therapy head of most lithotripters is continuously recirculated and degassed to take away any bubbles that might intervene with the shock-wave propagation. A coupling agent such as gel or oil is used to marry the rubber membrane of the treatment head to the skin [66].
Cheap amantadine 100 mg onlineConclusions Septic issues in genitourinary surgery are a lifethreatening state of affairs that urologists want to antiviral soap purchase amantadine 100mg mastercard avoid throughout their follow. Reduction in surgical antimicrobial prophylaxis expenditure and the speed of surgical web site infection via a protocol that controls the use of prophylaxis. Workgroup: Antimicrobial prophylaxis for surgery: an advisory assertion from the National Surgical Infection Prevention Project. Extracorporeal shock wave lithotripsy 25 years later: Complications and their prevention. Fever after shockwave lithotripsy: risk components and indications for prophylactic antimicrobial therapy. Incidence and risk elements of bacteriuria after transurethral resection of the prostate. The postoperative bacteriuria score: A new way to predict nosocomial infection after prostate surgical procedure. Antibiotic prophylaxis for transurethral prostatic resection in males with preoperative urine containing lower than one hundred,000 bacteria per ml: a scientific evaluation. Severe sepsis and septic shock: Review of the literature and emergency department management tips. Evidence based prescription of antibiotics in urology: a 5-year review of microbiology. Discarding antimicrobial prophylaxis for transurethral resection of bladder tumor: A feasibility examine. Mid stream urine C&S check is a poor predictor of contaminated urine proximal to the obstructing ureteric stone or contaminated stones: a potential medical examine. Stone and pelvic urine tradition and sensitivity are higher than bladder urine as predictors of urosepsis following percutaneous nephrolithotomy: A potential scientific research. Does a smaller tract in percutaneous nephrolithotomy contribute to high renal pelvic stress and postoperative fever Interaction of intracorporeal lithotripters with Proteus mirabilis inoculated inside artificial calcium and struvite stones. Inactivation of bacteria inoculated inside urinary stones-phantoms using intracorporeal lithotripters. Percutanoeus nephrostomy versus ureteral stents for diversi�n of hydronephrosis caused by stones: A potential, randomized medical trial. Perioperative antimicrobial prophylaxis in transperitoneal tumor nephrectomy: does it decrease the rate of clinically significant postoperative infections Antimicrobial prophylaxis in radical prostatectomy: 1-day versus 4-day remedies. Single-dose orally administered quinolone seems to be enough antibiotic prophylaxis for radical retropubic prostatectomy. Infectious issues in sufferers with chronic bacteriuria undergoing major urologic surgical procedure. Factors predisposing to urinary tract infections after J ureteral stent insertion. Procalcitonin as a diagnostic check for sepsis in critically ill adults and after surgery or trauma: A systematic evaluation and meta-analysis. This chapter addresses anticoagulants and the administration of patients on anticoagulants for specific urologic problems and procedures. In order to adequately perceive the mechanism of action of the anticoagulants, a quick evaluate of the hemostasis and coagulation cascade is necessary. Hemostasis requires applicable operate of four key components: platelet activation and aggregation, the clotting cascade, termination of clot formation, and fibrinolysis. Normal hemostasis Normal hemostasis requires a physiologic steadiness between prothrombotic and anticoagulant factors. Vascular damage results in the initiation of clotting and relies on three components: the vascular wall, platelets, and the coagulation cascade [1]. This is completed in three steps: adhesion, aggregation, and the secretion of procoagulant proteins that work together between platelets and endothelial cells, as well as between particular person platelets. The second essential step in thrombosis is the initiation of the coagulation cascade. The coagulation cascade is a series of steps in which proenzymes are transformed to activated enzymes, and the ultimate product is fibrin. At the site of vascular harm, the extrinsic pathway is initiated, beginning with the discharge of tissue factor from endothelial cells. Factors Xa and Va represent a last widespread pathway for each the extrinsic and intrinsic pathways. Many of the proenzymes within the coagulation cascade are dependent upon vitamin K as a cofactor, and subsequently antagonists corresponding to warfarin will disrupt the coagulation course of. Drug-mediated anticoagulation Warfarin Warfarin is a vitamin K-dependent anticoagulant. This pathway causes oxidative discount of vitamin K, which then permits for carboxylation of clotting elements from their inactive to active form. Therefore, warfarin administration results in the shortcoming to synthesize lively vitamin K-dependent clotting factors. The results of this could be a delayed effect of antithrombotic activity until pre-existing energetic clotting factors are expended. Careful monitoring of warfarin levels is mandatory as many variables can influence the efficacy of a given dose. These variables embrace vitamin K stores/intake, medical conditions (liver disease, thyroid disease, an infection, fever, heart failure), and medicines (quinolones, antifungals, trimethoprim�sulfamethoxazole, amiodarone, rifampin, barbiturates, levothyroxine, metronidazole). It can be given as both intravenous and subcutaneous injection, and subsequently anticoagulation administration may be performed as an outpatient directed by the clinician. That incidence increases to as excessive as 50% in the first three months after an initial event [4]. In 2008 the American College of Chest Physicians launched guidelines concerning management of those patients talking vitamin K antagonists [5, 6]. Patients have been stratified based on threat (high, reasonable, low) of both arterial or venous thromboembolic occasion primarily based on the underlying need for anticoagulation (Table 5. Those sufferers with a risk greater than 10%/year of a thromboembolic occasion were thought of high threat. Those patients with greater risk scores usually have a tendency to have thromboembolic occasions [7]. Great caution must be taken when withdrawing and restarting warfarin remedy in sufferers with sure conditions with identified risk of thromboembolism, together with antiphospholipid circumstances, and protein C and protein S deficiencies [8]. Rates of stent thrombosis are generally low, nevertheless the risk of thrombotic occasion after placement of drug-eluting stents is highest in these sufferers in whom clopidogrel has been discontinued [9]. There are numerous pointers relating to indications for use of these medicines for prevention; nevertheless, in general, sufferers utilizing this class of medicine for prevention of coronary artery disease are at low risk for complications if the treatment is stopped during intervention. In distinction, patients with coronary artery stents could also be at risk for stent thrombosis when anticoagulant remedy is stopped [3]. Guidelines Management of anticoagulation in the perioperative interval requires an understanding of the underlying pathologic state requiring anticoagulation. If that procedure has a threat of being combined with a further cystoscopic or ureteroscopic intervention, then the chance evaluation of anticoagulation ought to be for the extra invasive process.
References - John PG, Rahman J, Payne CB. Pulmonary hyalinizing granuloma: an unusual association with multiple sclerosis. South Med J 1995;88:1076-7.
- Biriukov YV, Streliaeva AV, Sadikov, et al. Obrabotka polosti kisti pri hidatidnom ehinokokoze (eksperimentalnoe-klinicheskoe izsledovanie). [Treatment of residual fibrous cavity in cystic echinococcosis (experimental and clinical study).] Hirurgia 2000; 27-29.
- Polat BE, Hart D, Langer R, Blankschtein D. Ultrasoundmediated transdermal drug delivery: mechanisms, scope, and emerging trends. J Control Release. 2011;152:330-348.
- Eckardt KU. Anaemia of critical illness?implications for understanding and treating rHuEPO resistance. Nephrol Dial Transplant. 2002;17(suppl 5):S48-S55.
- Hardell L, van Bavel B, Lindstrom G, et al: Increased concentrations of polychlorinated biphenyls, hexachlorobenzene, and chlordanes in mothers of men with testicular cancer, Environ Health Perspect 111:930n934, 2003.
|


