|
Dr Craig Davidson - Director Lane Fox Respiratory Unit
- Guys & St Thomas� Foundation Trust
- London
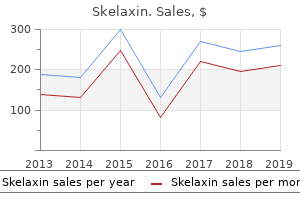
Skelaxin dosages: 400 mg
Skelaxin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills

Cheap 400mg skelaxin fast deliveryThe following equation is used to calculate creatinine clearance in mL/min when the serum creatinine focus is known: Clcr = Clcr = price of urinary excretion of creatinine serum concentration of creatinine CuV � a hundred Ccr � 1440 (24 spasms between ribs 400 mg skelaxin with amex. In a affected person with decreased glomerular filtration, serum creatinine will accumulate in accordance with the degree of loss of glomerular filtration within the kidney. The serum creatinine concentration alone is frequently used to determine creatinine clearance, Clcr. Creatinine clearance from the serum creatinine concentration is a rapid and convenient approach to monitor kidney perform. Creatinine clearance could also be defined as the volume of plasma cleared of creatinine per unit time. In practice, the serum creatinine concentration is determined on the midpoint of the urinary assortment period and the rate of urinary excretion of creatinine is measured for the complete day the place Ccr = creatinine concentration (mg/dL) of the serum taken at the 12th hour or on the midpoint of the urine-collection period, V = quantity of urine excreted (mL) in 24 hours, Cu = focus of creatinine in urine (mg/mL), and Clcr = creatinine clearance in mL/min. A small fraction of creatinine also is eliminated by active secretion and a few nonrenal elimination. Creatinine clearance values must be thought-about fastidiously in particular populations corresponding to aged, obese, and emaciated patients. In elderly and emaciated patients, muscle mass could have declined, thus lowering the production of creatinine. However, serum creatinine focus values could seem to be within the normal vary because of decrease renal creatinine excretion. Thus, the calculation of creatinine clearance from serum creatinine might give an inaccurate estimation of the renal function. Women with normal kidney operate have smaller creatinine clearance values than males, which are roughly 80%�85% of these in men with regular kidney perform. As a convenient approximation, the conventional clearance has typically been assumed by many clinicians to be approximately a hundred mL/min. Several methods are available for the calculation of creatinine clearance from the serum creatinine focus. These methods must be used just for sufferers with intact liver perform and no abnormal muscle disease, similar to hypertrophy or dystrophy. Cockcroft and Gault (1976) compared their method with the nomogram technique in adult males of various ages. Both methods also demonstrated an age-related linear decline in creatinine excretion, which may be because of the decrease in muscle mass with age. Calculation of Creatinine Clearance from Serum Creatinine Concentration the problems of obtaining a whole 24-hour urine collection from a affected person, the time necessary for urine assortment, and the evaluation time preclude a direct estimation of creatinine clearance. Serum creatinine concentration, Ccr, is related to creatinine clearance and is measured routinely in the scientific laboratory. Children There are a selection of methods for calculation of creatinine clearance in youngsters, based mostly on physique length and serum creatinine focus. Turn the best part of the ruler to the suitable serum creatinine value and the left facet will indicate the clearance in mL/min. What is the creatinine clearance for a 25-yearold male affected person with a Ccr of 1 mg/dL What is the creatinine clearance for a 25-yearold male patient with Ccr of 1 mg/dL and a physique weight of 80 kg Connect the intersection point at Solution the affected person is overweight and the Clcr calculation ought to be based mostly on best body weight. In acute renal failure and in different situations by which kidney perform is altering, the serum creatinine may not characterize steady-state situations. If Ccr is measured daily and the Ccr worth is fixed, then the serum creatinine concentration might be at steady state. Although the Cockcroft�Gault methodology for estimating Clcr has some biases, this methodology has gained common acceptance for the determination of renal impairment (Schneider et al, 2003; Hailmeskel et al, 1999; Spinler et al, 1998). A advised representation of sufferers with numerous degrees of renal impairment based mostly on creatinine clearance is shown in Table 24-3. The apply issues present that, depending on the formulation used, the calculated Clcr can vary considerably. Consequently, except a clinically important change in the creatinine clearance occurs, dosage adjustment may not be needed. For aminoglycosides and vancomycin, dose adjustment is individualized according to the wide range of Clcr. Each equation for the calculation of renal perform from serum creatinine concentrations provides somewhat totally different outcomes. The Cockcroft�Gault technique for estimating Clcr has been used most frequently and tends to be the popular method presently. These estimation methods are referred to as creatinine-based methods within the scientific literature (Stevens et al, 2006; Levey et al, 2009). The Cockcroft�Gault has a longer historical past of use but the authentic equation was based on fewer subjects. The Cockcroft�Gault formulation was developed initially with the information from 249 men with Clcr starting from 30 to one hundred thirty mL/min. Typically, regular values for creatinine clearance are normalized by a physique surface space of 1. For many new drugs, drug dosing data for renal-impaired sufferers is now available and must be consulted within the bundle insert. In patients with continual kidney disease, the next recommendations are good practices that physicians and pharmacists should concentrate on (Munar and Singh, 2007): 1. Use warning for medication with energetic metabolites that can exaggerate pharmacologic effects in patients with renal impairment. Whether renal impairment will alter the pharmacokinetics of the drug sufficient to justify dosage adjustment is a vital consideration. For many medicine that are eradicated primarily by metabolism or biliary secretion, uremia may not alter pharmacokinetics sufficiently to warrant dosage adjustment. Active metabolites of the drug can also be fashioned and must be thought-about for added pharmacologic effects when adjusting dose. For some 786 Chapter 24 drugs, the free drug concentrations may have to be considered because of decreased or altered protein binding in uremia. Combination merchandise that include two or extra energetic medication in a fixed-dose mixture could additionally be differentially affected by decreased renal perform and thus, using combination drug products in uremic patients ought to be discouraged. The following strategies could also be used to estimate initial and maintenance dose regimens. After initiating the dosage, the clinician should continue to monitor the pharmacodynamics and pharmacokinetics of the drug. As discussed by Chennavasin and Brater (1981), each nomogram has errors in its assumptions and drug database. In the uremic affected person, the speed of renal drug excretion has decreased, resulting in a decrease in complete body clearance. The fraction of normal renal function remaining in the uremic affected person is estimated from Clcr. After the remaining whole physique clearance within the uremic patient is estimated, a dosage regimen may be developed by (1) lowering the upkeep dose, (2) rising the dosage interval, or (3) altering both maintenance dose and dosage interval. Although whole physique clearance is a more accurate index for drug dosing, the elimination half-life of the drug is extra generally used for dose adjustment because of its convenience.
Order generic skelaxin lineThe pathophysiology is usually attributed to continual scarring from marginal ulcerations spasms going to sleep buy cheap skelaxin 400mg. This affected person offered with weight achieve 20 months after successful adjustable gastric band placement regardless of growing band quantity. The patient was diagnosed 5 days after Roux-en-Y gastric bypass with a leak at the gastrojejunal anastomosis. The affected person tolerated a transparent liquid diet the subsequent morning and was superior to an everyday diet per regular postoperative protocols without further incident. Six years after successful adjustable gastric band placement this patient developed heartburn unresponsive to proton pump inhibitor therapy. This affected person, who underwent a vertical banded gastroplasty, experienced important weight reduction, which was maintained for 20 years. Conversion to a Roux-en-Y gastric bypass resulted in resolution of symptoms and weight reduction to a body mass index of 24. This patient was unable to progress to strong meals 1 month after operation due to heartburn, nausea, and vomiting. Four years after adjustable gastric banding this affected person offered with growing reflux unresponsive to maximum doses of proton pump inhibitors, antacids, and sucralfate. After 2 years, however, the sense of restriction subsided and the affected person experienced weight regain. Dilatation of the ileoileal anastomosis and the proximal biliopancreatic limb is obvious. This affected person offered 2 weeks after the procedure with nausea and vomiting whereas not following the prescribed liquid diet. An arrow demonstrates medial dissection of distinction across the lower margin of this band. This affected person with wonderful initial weight reduction began having emesis and weight regain within the second postoperative year. With removal of the band the emesis resolved, however the patient experienced a rapid return to prebanded weight. Fat stranding is noted and fluid collection within the anterior belly wall communicates with small bowel. A protracted postoperative course, together with drainage and parenteral nutrition, resulted in eventual resolution 3 months after ileoileal anastomotic revision. An enterotomy was closed in the medial facet of the staple line on repeat laparoscopy. Profound dilation of the esophagus and stomach pouch with trickling of contrast past the anastomosis is shown. This patient progressed initially to semisolid meals, however four weeks after Roux-en-Y gastric bypass began having intermittent, but progressive nausea and vomiting. A distinction examine was performed in clinic 7 weeks after the operation as a end result of the patient was tolerating solely clear liquids. Then, a lined self-expanding Nitinol stent is fastidiously deployed, again with position affirmation via fluoroscopy. Contrast study should be carried out prior to stent elimination, at about 6 weeks on the earliest. These pathogens are thought-about opportunistic in immunosuppressed persons as a outcome of they happen more regularly, trigger more severe illness, and are associated with more extended or recurrent an infection. Gastrointestinal complications are additionally related to allogeneic hematopoietic stem cell and strong organ transplantation. Graft-versus-host disease, which have to be differentiated from infectious processes, is the most typical gastrointestinal complication of hematopoietic stem-cell transplantation. Opportunistic enteric infections, notably cytomegalovirus, also commonly complicate solid organ transplantation. Cytomegalovirus induction of tumor necrosis facor- by human monocytes and mucosal macrophages. Cytomegalovirus induction of tumor necrosis factor- by human monocytes and mucosal macrophages. Histopathology of tissue obtained by biopsy of the rectal ulcer proven in the figure revealed ulceration with dense infiltration by persistent inflammatory cells and focal areas of acute irritation. Strand displacement amplification of material obtained by rectal swab was positive for C. Gastrointestinal involvement normally signifies disseminated an infection and is related to diarrhea, weight reduction, fever, and a excessive bacterial burden in tissues. The image reveals multiple small yellow plaques, a few of which have coalesced in the second portion of the duodenum. Liver biopsy exhibits macro- and microvesicular steatosis without cholestasis (magnification �20). In addition to hepatic steatosis, these brokers have been occasionally related to myopathy, kind B lactic acidosis, and fulminate hepatic failure. The scientific features of intestinal illness embody watery diarrhea, anorexia, nausea, vomiting, stomach ache, and bleeding. Intestinal biopsy from a patient with graft-versus-host illness shows flattening of crypts, crypt degeneration, edema, ulceration (magnification �20) (top right) and typical epithelial cell apoptosis with (arrow) apoptotic our bodies, necrotic epithelial cells, and minimal inflammatory cell infiltration (magnification �40). The gastrointestinal tract is a main target organ in each major and secondary immunodeficiency problems because of its massive floor space and fixed exposure to environmental pathogens. The gut mucosa is composed of the only largest collection of lymphoid tissue within the physique, primed to respond effectively to microbial challenge while at the identical time regulated closely to avoid inappropriate and doubtlessly harmful immune responses to the extensive and diversified exposures experienced at this host�environment interface. The principal gastrointestinal consequence of immunodeficiency is increased susceptibility to an infection. This contains an infection with unusual agents, atypical manifestations of an infection with commonly encountered pathogens, and bacterial overgrowth with organisms usually current within the gastrointestinal tract. There is also an elevated prevalence of autoimmune disorders or continual inflammatory situations such as atrophic gastritis, inflammatory bowel disease, and celiac illness. Benign diffuse nodular lymphoid hyperplasia might happen amongst some sufferers, whereas lymphoid atrophy may be a feature amongst others. Patients with severe immunodeficiency could have graft-versus-host disease caused by transplacentally acquired maternal lymphocytes or unintentional transfusion of nonirradiated blood merchandise. However, patients with delicate or selective types of immunodeficiency, corresponding to selective IgA deficiency, incessantly are free of infections or different manifestations. They are most prevalent within the small bowel, in some cases extend into the colon, and rarely lengthen into the stomach. Among sufferers with selective immunoglobulin A (IgA) deficiency, the absence or paucity of IgA-producing cells is compensated for by a rise in IgM-producing cells. It happens most incessantly amongst patients with common variable hypogammaglobulinemia. Although the analysis of giardiasis may be created from inspection of histological sections of small bowel, finding the organism by means of this method is troublesome and tedious when the infection burden is low. The prognosis is made extra conveniently by examination of the stools for cysts, or identification of the trophozoite type in intestinal fluid or smears of mucus adherent to the biopsy specimen. Lymphoid hyperplasia is believed to be caused by proliferation of B cells which may be unable to endure full differentiation to immunoglobulin secretion and subsequently are unresponsive to suggestions regulation of proliferation.
Diseases - Juberg Marsidi syndrome
- Lipomatosis familial benign cervical
- Aloi Tomasini Isaia syndrome
- Tricho-hepato-enteric syndrome
- Hidradenitis suppurativa
- Charcot Marie Tooth disease, X-linked type 3, recessive
- Endocarditis, infective
- Hyperbilirubinemia type 2
- Morquio disease, type B
Cheap skelaxin expressThe state of affairs has now modified muscle relaxant cyclobenzaprine high order cheap skelaxin on-line, recent research having demonstrated the efficacy of newer targeted therapies and immunotherapy in patients with melanoma mind metastases. Now, more than ever, medical trials are needed in patients with active brain metastases. In this part new systemic therapies for metastatic melanoma and their evolving function in the administration of brain metastases (see Table 5. A randomized section three study of fotemustine together with forty three sufferers with energetic mind metastases demonstrated a I. Cohort A included 89 sufferers who had not acquired earlier native therapy and cohort B enrolled eighty three sufferers whose mind metastases had progressed after prior local therapy. The world illness management fee was roughly 80% for these with V600E and 50% for sufferers with V600K mutations. The toxicities had been as anticipated based on previous trials of dabrafenib (Falchook et al. The number of intracranial hemorrhages was decrease than the reported price of spontaneous hemorrhage (up to 40%) for melanoma brain metastases (Raizer et al. The examine showed a safety profile consistent with earlier expertise with vemurafenib, together with toxicities similar to arthralgia, rash, cutaneous squamous cell carcinomas, and photosensitivity. These results have to be interpreted with warning as the research was very small, retrospective, and lots of sufferers underwent pretreatment with neurosurgery and/or systemic remedy. Additionally, radiosensitization and radiation recall have been reported at extracranial sites handled with radiotherapy in sufferers receiving vemurafenib (Anker et al. Preclinical studies have demonstrated higher brain penetration of dabrafenib compared with vemurafenib (Mittapalli et al. None of the trials to date have included patients with active mind metastases, however a phase 2 trial of combination dabrafenib and trametinib remedy in this setting is deliberate Table 5. A retrospective sequence showed some activity in these with pretreated brain metastases but little benefit in a previously untreated cohort (Guirguis et al. In a section 2 trial seventy two sufferers with melanoma brain metastases had been handled with initial induction of four infusions of ipilimumab 10 mg/kg each three weeks followed by 12 weekly upkeep infusions in sufferers who have been clinically steady at 24 weeks (this differs from the currently accredited dose and schedule for ipilimumab in many countries). Patients had been enrolled in two cohorts; cohort A consisted of patients with asymptomatic mind metastases and cohort B consisted of patients requiring steroid remedy to management neurologic symptoms or cerebral edema. The most common adverse events included fatigue, diarrhea, nausea, headache, rash, and pruritus, in keeping with earlier expertise with ipilimumab (Hodi et al. Blocking this interplay prevents inactivation of T cells on the tumoral degree and augments the antitumor immune response. Suggested Approach to Management A advised strategy to administration of sufferers with melanoma brain metastases, incorporating local and systemic therapies, was revealed recently (Lyle and Long, 2014). Enrolment in a medical trial, if obtainable, is really helpful for all sufferers with metastatic melanoma. Management must be mentioned by a multidisciplinary group, with consultation between surgical oncologists, neurosurgeons, radiation oncologists, medical oncologists, and others involved in patient care. The beneficial management of mind metastases must be based on a range of factors together with mutation standing, performance status, price of progression, presence of signs, and extent of extracranial illness. However, the possibly unfavorable impression of steroid therapy on the activity of ipilimumab (Margolin et al. It is obvious that optimal therapy outcomes require Multidisciplinary care, with built-in and acceptable sequencing of surgical procedure, radiation therapy and systemic therapies. More analysis is required to further enhance patient outcomes, and strategies to investigate the exercise of latest therapies in active brain metastases have to be considered at an early stage in drug growth. Severe liver and pores and skin toxicity after radiation and vemurafenib in metastatic melanoma. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for therapy of brain metastases: a randomized managed trial. High-dose recombinant interleukin-2 remedy in patients with metastatic melanoma: long-term survival update. Should prophylactic anticonvulsants be administered to sufferers with newly-diagnosed cerebral metastases Prognostic factors for survival after stereotactic radiosurgery vary with the number of cerebral metastases. A randomized, blinded, placebo-controlled trial of divalproex sodium prophylaxis in adults with newly recognized mind tumors. Safety and efficacy of high-dose interleukin-2 therapy in sufferers with mind metastases. Vemurafenib in metastatic melanoma sufferers with brain metastases: an open-label, single-arm, part 2, multicenter research. Stereotactic radiosurgery in the treatment of mind metastases: the present proof. Ipilimumab in sufferers with melanoma and mind metastases: an open-label, phase 2 trial. Gamma knife radiosurgery within the administration of malignant melanoma brain metastases. Mechanisms limiting distribution of the threonine-protein kinase B-RaF(V600E) inhibitor dabrafenib to the mind: implications for the treatment of melanoma mind metastases. Melanoma of the central nervous system: report of thirty-four circumstances, in nineteen of which the prognosis was verified by operation or necropsy. Reevaluation of surgery for the therapy of mind metastases: evaluation of 208 patients with single or a number of mind metastases handled at one establishment with trendy neurosurgical strategies. Brain and leptomeningeal metastases from cutaneous melanoma: survival outcomes primarily based on scientific features. Treatment of 283 consecutive sufferers with metastatic melanoma or renal cell cancer using high-dose bolus interleukin 2. Demographics, prognosis, and therapy in 702 sufferers with mind metastases from malignant melanoma. Stereotactic radiosurgical remedy in 103 sufferers for 153 cerebral melanoma metastases. Radiosurgery for brain metastases: relationship of dose and sample of enhancement to native control. Cranial irradiation after surgical excision of brain metastases in melanoma patients. They reach the mind both from hematogenous unfold or through direct invasion from adjacent tissues. They comprise about 25% of all most cancers metastases and may be seen in about 20�40% of all adult most cancers sufferers. The variety of instances for the positioning of origin is 40�50% for lung, 15�20% for breast, 5�10% for pores and skin, and 4�6% for the gastrointestinal tract (Barnholtz-Sloan et al. Brain metastases are the leading reason for morbidity and mortality in most cancers sufferers. Median survival time for untreated sufferers is 5 weeks; multimodality remedy may prolong survival to 3�18 months (McDermott et al.
Skelaxin 400 mg low costBoth in emergency and in day by day apply muscle relaxant dosage flexeril purchase skelaxin 400mg without a prescription, gastroenterologists are increasingly encountering bariatric patients and should be in a position to handle the most incessantly encountered problems. Vertical banded gastroplasty, nonetheless a primary operation in some areas, has largely been changed by the gastric sleeve and adjustable gastric band. The adjustable gastric band and gastric sleeve have turn into popular restrictive operations in its place. Also offered is a super morbidly obese affected person who had a biliopancreatic diversion with duodenal change. In spite of reoperation and a difficult recovery interval, this patient had glorious weight reduction and full resolution of comorbidities. Although biliopancreatic diversion with duodenal switch has a higher complication fee than the opposite main procedures, its higher weight reduction and resolution of comorbidities make it a serious choice in many severely obese sufferers, even these sufferers with a physique mass index under 50. A circumferential ulcer is seen entirely on the jejunal aspect of the gastrojejunal anastomosis. This affected person introduced 6 weeks after Roux-en-Y gastric bypass with growing quantity depletion secondary to poor oral consumption with a big marginal ulcer on endoscopy. For prevention, avoidance of nonsteroidal antiinflammatory medicine and tobacco in the perioperative period can be strongly recommended. This affected person experienced progressive postprandial nausea and vomiting 1 month postoperatively. Nodular lymphoid hyperplasia could additionally be asymptomatic, however may be associated with bleeding, pain, diarrhea, and, when very massive, obstructive symptoms. It is essential to recognize that localized types of nodular lymphoid hyperplasia, particularly in the massive bowel, may happen amongst apparently wholesome immunocompetent persons. Small nodules of lymphoid tissue on a background of regular folds of small bowel are regular and are a common discovering among youngsters and younger adults. Immunodeficiency brought on by enteric protein loss could additionally be a part of any extreme inflammatory dysfunction of the gastrointestinal tract. The most extreme instances of gastrointestinal protein loss happen with lymphangiectasia, which may be major or secondary to lymphatic obstruction. Protein loss from the gastrointestinal tract is nonselective, and hypogammaglobulinemia is at all times accompanied by hypoalbuminemia. The absence of plasma cells within the lamina propria is notable here and is a characteristic suggestive of primary immunodeficiency. Histological options are much like features in immunocompetent affected people, but delicate differences, similar to diminishment in plasma cell numbers in the lamina propria, might occur. Antiinflammatory and immunosuppressive therapy could additionally be required to control the process in some sufferers. Graft-versus-host disease Gastrointestinal complications happen among virtually all sufferers at some stage throughout restoration from bone marrow transplantation. In addition to graft-versus-host disease, causes of gastrointestinal signs after bone marrow transplantation embrace the effects of chemotherapy and chemoradiation remedy given earlier than bone marrow grafting and opportunistic infections that could be caused by the immunosuppressive protocol or the immunodeficiency associated with graft-versus-host disease. The gastrointestinal and liver injury associated with chemoradiation therapy usually resolves within 20�30 days after transplantation. Opportunistic infections may occur at any stage after bone marrow transplantation; bacterial and fungal infections are most likely to be extra frequent during the first month and viral infections more common thereafter. The scientific severity and extent of gastrointestinal involvement with acute and persistent graft-versus-host disease are highly variable. Acute graft-versus-host disease usually happens 20�60 days after transplantation and primarily impacts the pores and skin, liver, and gastrointestinal tract. Chronic graft-versus-host disease is a multisystem dysfunction with medical features resembling these of sicca syndrome and systemic sclerosis. Gastrointestinal involvement is particularly widespread in the oral mucosa (mucositis), esophagus, and small bowel. Chronic graft-versus-host disease often happens 80�400 days after transplantation. This characteristic discovering is diagnostic if obtained from normalappearing mucosa at least 20 days after transplantation (when the consequences of chemoradiation therapy have resolved). The particular person crypt cell apoptosis (karyolytic debris in vacuoles near crypt base) is characteristic if found after day 20, when injury from chemoradiation remedy has resolved. The radiographic look of graft-versus-host disease additionally varies with the severity and with the stage of the illness. The notable features are the diffuse bowel wall thickening, luminal extra fluid, and mucosal hyperenhancement following distinction. The endoscopic look of acute graft-versus-host disease could also be normal, present patchy erythema, or present intensive mucosal sloughing, notably in the ileum, cecum, and ascending colon, with relative sparing of the rectal and gastric mucosa. In distinction, esophageal involvement is especially frequent in continual graft-versus-host illness. Lesions include desquamation of the upper esophagus and upper esophageal webs; the distal esophagus normally is spared. Infected macrophages also may be seen in the lamina propria, whereas epithelial cells are seldom concerned. Infestation with Entamoeba histolytica, the causative agent of amebic dysentery and amebic liver abscess, is primarily a illness of creating nations. Infestation with Giardia lamblia, Cryptosporidium parvum, and Cyclospora cayetanensis, however, poses serious threats to public well being in the United States and the the rest of the world. Physicians (gastroenterologists in particu lar) should consider these pathogens within the differential prognosis of acute and persistent diarrhea and ought to be acquainted with the optimal diagnostic Table sixty six. Because conventional microscopic examination of the stool for ova and parasites is time consuming and expen sive, particular requests for microscopic examinations may need to be made to the laboratory. In some hospitals, only fecal immunoassay(s) directed in opposition to Giardia and Cryptosporidium species could additionally be carried out when stool ova and parasite testing is requested. Patients normally have the triad of fever, proper upper quadrant pain and tenderness, and a spaceoccupying lesion within the liver. Amebiasis Improved sanitation situations have tremendously lowered the variety of cases of amebiasis within the United States. Disease in the United States might be mostly detected amongst immigrants and must be thought-about for all individuals with dys entery and an appropriate travel or exposure historical past. Groups at excessive risk for giardiasis embody youngsters in daycare facilities and their grownup contacts, travelers, and those who eat contami nated water. Type of parasite Extracellular ameboid Entamoeba histolytica Stool Intestinal biopsy Blastocystis hominis (pathogenicity is controversial) Flagellates Giardia lamblia Trophozoite 10�20 m with pale, round nucleus with small central karyosome; cyst 9�25 m with four nuclei Morphologically indistinguishable from Entamoeba dispar; immunoassays for detection of trophozoite antigen can differentiate E. This trophozoite is approximately 20 m in diameter and has the characteristic spherical nucleus with a small, centrally positioned karyosome. Elevated proper hemidiaphragm, pleural effusion, and basilar infiltrate are depicted. Symptoms ascribed to this organism embrace gentle diarrhea, abdominal ache, anorexia, and fatigue. Numerous large trophozoites within the wall of the gut in a patient with acquired immunodeficiency syndrome.
Trusted skelaxin 400mgIn contrast spasms head order skelaxin 400 mg with amex, for melanoma solely performance standing and the number of mind metastases seems prognostic (Sperduto et al. The vast majority of the patients treated for brain metastases from gynecologic malignancies have been treating utilizing various iterations of the Gamma Knife system (Lee et al. Rigid immobilization of the goal permits for the maximum diploma of accuracy and precision when treating intracranial lesions. At our institution this is sometimes carried out with the utilization of native anesthetic at the pin sites and intravenous sedation. The entire mind is imaged with a contrast-enhanced thin-sliced (2-mm thick photographs with none gap) T1-based protocol. Often T2-weighted pictures are additionally obtained so as to higher respect tumor margins and determine reactive modifications. These pictures are then imported into the radiosurgical treatment planning software program. Historically, dose choice has been primarily based to a point on the findings of the Radiation Therapy Oncology Group study 90-05 (Shaw et al. The out there literature for ovarian and endometrial cancers signifies that median doses from 16 Gy to 20 Gy are typically utilized (Menendez et al. Prescription dose can be decreased 2�4 Gy when patients are handled for lots of lesions. Each tumor is then moved into the path of the centered 192 or 201 beams, relying on the specific unit, until the prescribed dose is achieved. Once all of the recognized tumors are treated, the patient is removed from the system and the stereotactic head frame is taken off. The patient is often discharged the same day because the process and can return to ordinary actions the following day. Axial contrast-enhanced magnetic resonance pictures with coronal and sagittal reconstructions have been utilized for planning. Four months after therapy, there was no proof of the tumor on computed tomography and on the time of publication the patient was without neurological symptoms or intracranial disease. Due to the epidemiology of ovarian cancer brain metastases, subsequent reports have been uncommon. As of 2011, Piura and Piura famous that only a complete of 520 patients had been included in reviews involving therapy of brain metastases from ovarian most cancers (Piura and Piura, 2011). The median survival of these sufferers had not been achieved by the point of publication. One affected person had an antagonistic radiation impact and required a craniotomy for radiation necrosis. In a research of the prognostic elements related to mind metastases from ovarian carcinoma, Kim et al. The median age at the time of treatment was 56 years with a median interval from the time of preliminary cancer diagnosis to findings of mind metastases of 28 months. Our group revealed the largest collection to date in 2008, which studied 21 patients with ovarian carcinoma (Monaco et al. Stereotactic photographs (A and B) have been obtained on the day of Gamma Knife and present moderately sized enhancing tumors. Two months after radiosurgery (C and D) the 2 tumors have dramatically responded with prominent decreases in measurement by quantity (arrows). The patient succumbed to her systemic illness 4 months after radiosurgery without neurological deficit. The median number of tumors handled was two and the median margin prescription dose was 20 Gy. In a sequence on the therapy of major cancers that rarely metastasize to the brain Menendez et al. No overall tumor control price was reported, nor was there mention of complications. The median marginal dose, which included remedy of eight further patients with distinct gynecological malignancies, was 20 Gy. There were no prognostic elements associated with improved survival in this cohort. This affected person was nonetheless alive at the time of publication with no reported proof of systemic or cranial disease. She was found to have a large left frontal brain metastases that was resection and he or she was referred for tumor mattress radiosurgery 1 month later. The tumor bed was handled with a prescription dose of 18 Gy to the 50% isodose line. Panel A is an image from the stereotactic examine performed on the day of Gamma Knife and reveals the tumor bed goal (arrow). Panel B is a follow-up image by way of the identical area obtained approximately 1 12 months later and shows no evidence of active illness on the tumor bed. In a sequence of 22 patients identified over a decade with endometrial carcinomas, Chura et al. The median prescription dose for all patients, including a quantity of with other gynecological malignancies, was 20 Gy. The actuarial survival for these sufferers was 50% at 6 months and 33% at 12 months. Uterine leiomyosarcoma is also exceedingly rarely reported to metastasize to the mind. The patient developed a brain lesion 3 years after systemic treatment with chemotherapy. She was still alive on the time of publication and her last consequence was not reported. Six months submit radiosurgery all tumors had regressed dramatically, however a new tumor was obvious. Longitudinal modifications in white matter disease and cognition within the first 12 months of the Alzheimer disease neuroimaging initiative. Stereotactic irradiation: potential new remedy methodology for brain metastases resulting from ovarian most cancers. Successful remedy of mind metastases from ovarian most cancers using gamma-knife radiosurgery. Prognostic elements related to brain metastases from epithelial ovarian carcinoma. Gamma-knife radiosurgery as an optimum therapy modality for mind metastases from epithelial ovarian cancer. Stereotactic radiosurgical treatment of brain metastasis of major tumors that hardly ever metastasize to the central nervous system. Management of mind metastases from ovarian and endometrial carcinoma with stereotactic radiosurgery. Leukoencephalopathy after whole-brain radiation therapy plus radiosurgery versus radiosurgery alone for metastatic lung cancer. Endometrial carcinoma with a predominant clear-cell pattern with metastases to the adrenal, posterior mediastinum, and brain. Gamma Knife radiosurgery as a primary therapy choice for solitary brain metastases from ovarian carcinoma.
Order 400 mg skelaxin amexTherefore spasms right flank order skelaxin 400mg on line, u the renal drug clearance, ClR, in the uremic patient is u ClR = u Clcr N � ClR Clcr u Clcr N Clcr (21. Alternatively, if the conventional whole physique clearance, Cl, and fe are recognized, Dose Adjustment in Renal and Hepatic Disease 795 Equation 24. A statistical strategy was utilized by Wagner (1975), who established a linear relationship between creatinine focus and the first-order elimination price constant of the drug in sufferers. The Wagner method is described in higher detail within the third version of this guide. This method takes benefit of the fact that the elimination fee fixed for a affected person can be obtained from the creatinine clearance, as follows: k% = a + b Clcr (23. The creatinine clearance on this affected person has decreased to a steady stage of 50 mL/min. The values of a and b are decided statistically for each drug from pooled data on uremic sufferers. The technique is simple to use and will present correct dedication of elimination price constants for sufferers when a great linear relationship exists between elimination rate constant and creatinine concentration. The theoretical derivation of this approach is as follows: k% = whole elimination rate constant knr = nonrenal elimination fee constant kr = renal excretion rate constant Cl = complete physique clearance of drug R= Cl Clcr Solution fe = 0. In such circumstances, the terminal half-life is used, and the terminal slope of the elimination curve (b) is substituted for 796 Chapter 24 the elimination rate constant k. Since the equation assumes a constant nonrenal elimination fixed (knr) and volume of distribution, any change in these two parameters will result in an error in the estimated elimination rate constant. Frequently Asked Questions �� What are the benefits and downsides of using serum creatinine concentrations for the measurement of renal operate Limitations of Dose Adjustment Methods in Uremic Patients All of the methods mentioned previously have similar limitations (see Table 24-2). For example, the drug must follow dose-independent kinetics and the volume of distribution of the drug should remain comparatively constant in the uremic affected person. Therefore, there are potential sedative side effects in the renally impaired patient as a result of the longer metabolite half-life. Bodenham and coworkers (1988) also cited literature references to potentiation of sedative and analgesic drug effects in renal, liver, and different multisystem illness states. Another assumption in the usage of these strategies is that pharmacologic response is unchanged within the uremic patient. This assumption could additionally be unrealistic for medication that act in a unique way in the illness state, and potential changes in pharmacodynamic effects in sufferers with renal and other diseases have to be thought-about. For example, the pharmacologic response with digoxin relies on the potassium degree in the physique, and potassium level within the uremic patient could also be rather different from that of the conventional particular person. In a affected person present process dialysis, lack of potassium could improve the potential for toxic impact of the drug digoxin. In addition, neuromuscular-blocking drugs could also be potentiated or antagonized by changes in potassium, phosphate, and hydrogen ion focus caused by uremic states, and morphine potentiation has been reported in hypocalcemic states. For many medicine, research have shown that the incidence of adverse results is elevated in uremic sufferers. It is usually inconceivable to distinguish whether or not the rise in opposed impact is as a outcome of of a pharmacokinetic change or a pharmacodynamic change in the receptor sensitivity to the drug. Serum creatinine concentration could not rise for a while till Clcr has fallen significantly, thereby including to the uncertainty of any method that is determined by serum Clcr for dose adjustment. In any event, these observations level out the truth that dose adjustment must be regarded as a preliminary estimation to be adopted with additional changes in accordance with the observed medical response. Several strategies are available for the extracorporeal removal of drugs, including hemoperfusion, hemofiltration, and dialysis. The objective of those strategies is Dose Adjustment in Renal and Hepatic Disease 797 to rapidly take away the undesirable medicine and metabolites from the body without disturbing the fluid and electrolyte stability within the patient. Patients with impaired renal perform may be taking different treatment concurrently. For these sufferers, dosage adjustment could also be wanted to replace drug loss throughout extracorporeal drug and metabolite removal. Dialysis Dialysis is a synthetic process by which the buildup of medication or waste metabolites is eliminated by diffusion from the body into the dialysis fluid. The dialysate incorporates water, dextrose, electrolytes (potassium, sodium, chloride, bicarbonate, acetate, calcium, etc), and different components similar to normal body fluids without the toxins. Peritoneal Dialysis Peritoneal dialysis uses the peritoneal membrane in the abdomen because the filter. However, solely a small portion of the total splanchnic blood flow (70 mL/min out of 1200 mL/min at rest) comes into contact with the peritoneum and gets dialyzed. The dialysis fluid is pumped into the peritoneal cavity, where waste metabolites in the physique fluid are discharged rapidly. The dialysate is drained and fresh dialysate is reinstilled after which drained periodically. However, slower drug clearance rates are obtained with peritoneal dialysis compared to hemodialysis, and thus longer dialysis time is required. Many diabetic sufferers turn into uremic on account of lack of control of their disease. About 2 L of dialysis fluid is instilled into the peritoneal cavity of the affected person via a surgically positioned resident catheter. The objective is to take away accrued urea and different metabolic waste within the body. Every 4�6 hours, the fluid is emptied from the peritoneal cavity and changed with fresh dialysis fluid. Hemodialysis Hemodialysis makes use of a dialysis machine and filters blood through a synthetic membrane. Hemodialysis requires entry to the blood vessels to allow the blood to circulate to the dialysis machine and again to the physique. For momentary access, a shunt is created within the arm, with one tube inserted into an artery and another tube inserted into a vein. For permanent access to the blood vessels, an arteriovenous fistula or graft is created by a surgical procedure to enable entry to the artery and vein. At the start of the hemodialysis process, an arterial needle allows the blood to flow to the dialysis machine, and blood is returned to the patient to the venous facet. During hemodialysis, the blood flows via the dialysis machine, where the waste materials is faraway from the blood by diffusion via an artificial membrane earlier than the blood is returned to the physique. Hemodialysis is a way more effective technique of drug removal and is most popular in situations when rapid elimination of the drug from the body is essential, as in overdose or poisoning. In follow, hemodialysis is most frequently used for sufferers with end-stage renal failure. Dialysis may be required from as soon as each 2 days to 3 times a week, with every remedy period lasting for 2�4 hours.
Flea Wort (Canadian Fleabane). Skelaxin. - What is Canadian Fleabane?
- Dosing considerations for Canadian Fleabane.
- Are there safety concerns?
- Bronchitis, diarrhea, dysentery, worms, fever, inflammation, swelling, bleeding from the uterus, sore throat, urinary tract infections (UTIs), and tumors.
- How does Canadian Fleabane work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96267
Purchase skelaxin torontoCholecystectomy for gallstone-induced acute pancreatitis must be performed using a laparoscopic process after resolution of acute pancreatitis spasms perineum generic skelaxin 400mg amex. After the first week, distinction between these two forms of collections is normally attainable. Cholelithiasis (*) and edematous (arrow) pancreas tissue with peripancreatic fluid areas are proven in anterior pararenal space at (a) arterial and (b) portal venous phases. Fine needle aspiration is helpful for verify prognosis and to get hold of a specimen for tradition. Classification of acute pancreatitis�2012: revision of the Atlanta classification and definitions by international consensus. Complications similar to bleeding, inadvertent puncture of adjacent viscera, secondary an infection, and prolonged intervals of drainage with resultant pancreaticocutaneous fistulae could also be avoided. The revised Atlanta classification of acute pancreatitis: its importance for the radiologist and its impact on treatment. Small-diameter plastic stents simply occlude, particularly with fluid collections containing particles. Stent occlusion might therefore lead to an infection and delayed decision of necrotic tissue. Moreover, surgical necrosectomy throughout the first weeks is associated with high mortality charges (up to 65%). Pancreas is changed by low-attenuation assortment with a well-defined rim and a number of pockets of fuel. Pancreatic trauma is rare and associated with harm to different higher abdominal viscera. Empiric antibiotics should embody each cardio and anaerobic Gram-negative and Grampositive microorganisms. All images present peripancreatic secretion accumulation (arrow) and rupture in the neck of the pancreas. In the past, parenteral diet appeared to be ideal for eliminating the stimulation of pancreatic secretion while stopping deterioration of nutritional standing and progression to protein vitality malnutrition. Complications embody formation of pseudocysts, pancreatic duct stenosis, duodenal stenosis, vascular problems, biliary obstruction, malnutrition, and a continual ache syndrome. Chronic pancreatitis can be a risk factor for the event of pancreatic cancer. The most typical explanation for an acute exacerbation of pancreatitis is continued alcohol abuse or dietary transgressions. Acute exacerbation of chronic pancreatitis manifests in two varieties, irrespective of underlying etiology: acute interstitial edematous pancreatitis (75%�85%) with a mortality of beneath 1%, and acute hemorrhagic necrotizing pancreatitis (15%�25%) with a mortality between 10% and 24%. Complications are frequent in sufferers with chronic pancreatitis, and pseudocysts are among the most common findings. Obstruction of the outflow of exocrine secretions both by an inflammatory mass, calcified protein plaques in pancreatic ducts, or narrowing of ducts by inflammatory scars usually causes continual ache. Gastric varices, particularly in the fundus, may develop as a end result of thrombosis of the portal vein or splenic vein. The inflammatory processes could result in a fistula, which may connect with the small or large bowel and trigger short bowel syndrome. Transabdominal ultrasound: dilated major pancreatic duct and protein plug within the duct (arrow). Transabdominal ultrasound: round, echo-poor liquid construction divided by a septum (arrow). Pancreatic pseudocysts are a frequent complication of acute and continual pancreatitis. Transabdominal ultrasound: acoustic reflections as a outcome of pancreatic parenchymal calcifications (arrows). Radial endoscopic ultrasound: acoustic parenchymal reflexes as a outcome of calcifications. Improvement of major pancreatic duct visualization after secretin stimulation (d, e, f). Morphology of pancreatic ducts corresponds to grade four in accordance with the Cambridge classification. Esophagogastroduodenoscopy: impression of the gastric lumen as a end result of a pancreatic pseudocyst. Esophagogastroduodenoscopy: the endoscope is retroflexed with view to the gastric fundus. Angiography: (a) small pseudoaneurysm caused extreme bleeding (arrow); (b) profitable treatment by coiling (arrow). Angiography: (a) proteolytic destruction of a giant pseudoaneurysm (arrow) of the gastroduodenal artery triggered life-threatening bleeding. Duodenoscopy: (a) spontaneous perforation of pancreatic necrosis into the distal duodenal bulb; evacuation of pus and necrotic materials. This gene encodes cationic trypsinogen, the principal trypsin proenzyme in human pancreatic juice. Together, the 12 helices (h1�h12) surround an aqueous pore, which forms a channel by way of the lipid bilayer and allows anions to passively move via the cell membrane. Common additional findings embrace neutropenia, and progress or skeletal abnormalities. Localization of the cystic fibrosis transmembrane conductance regulator in pancreas. Localization of the cystic fibrosis transmembrane conductance regulator in human bile duct epithelial cells. As pancreatic juice flows via the intralobular duct, the protein-rich acinar secretions are diluted and alkalinized by the duct epithelial cells. This atrophic gland is fibrotic and exhibits prominent lobulation with cystic modifications. Typical findings embody focal portal and periportal fibrosis, ductular proliferation, and periductular irritation. Proximal to this obstruction, the small bowel is distended (note thickened bowel wall and gasoline bubbles in fecal material). Much of the mucosal surface is covered with concretions consisting of inspissate mucofecal materials. If active trypsin accumulates in the pancreatic parenchyma, this potentially might trigger an uncontrolled proteolytic chain reaction because extra activated trypsin could be produced by the action of trypsin on trypsinogen. To stop this, trypsinogen usually contains an inactivating cleavage site at an accessible web site on its floor (R122). In hereditary pancreatitis, the R122H mutation prevents digestion of trypsinogen at R122 and this enables lively trypsin to accumulate in an uncontrolled manner. Thus, excessive activation of trypsin is believed to be the first event inflicting pancreatic injury in many patients with hereditary pancreatitis. The pancreas reveals adjustments in keeping with persistent pancreatitis including delicate atrophy and a number of punctate parenchymal calcifications (especially in the pancreatic head). Typical exocrine gland features embody fatty substitute of acini with sparing of ducts. Steatorrhea and diabetes mellitus usually happen two to 4 decades after the onset of pancreatitis, whereas pancreatic most cancers is normally delayed by a further two to three decades.
Buy 400 mg skelaxin mastercardThe equation represents the least-squares estimation of the concentration by minimizing deviation squares (first summation term of Equation 22 muscle relaxant m 751 buy skelaxin 400mg visa. The intersubject variation, intrasubject variance, and random error have to be minimized properly to allow environment friendly parameter estimation. There is a series of inhabitants parameters in the model for the ^ kth population parameter, Pk Pk is the estimated inhabitants parameter and hk is the kth parameter 2 random error with variance of k. To examine the performance of the Bayesian technique to other strategies in drug dosing, Sheiner and Beal (1982) generated some theophylline plasma drug concentrations based mostly on known clearance. They added various error levels to the information and divided the patients into teams with one and two plasma drug samples. The information were then analyzed using the Bayesian method and a second (alternative) method in figuring out the pharmacokinetic parameter (ClT). The success of the Bayesian approach is due to the ability of the 718 Chapter 22 A (0. A more precise clearance estimation will lead to extra correct dose estimation within the affected person. All ratios are divided by the proper ratio so that a value of unity D signifies that the proper ratio itself was used. Application of Pharmacokinetics to Clinical Situations 719 assumptions in regards to the imply and normal deviation of the distribution. Generally, finding a set of finest parameter estimates to describe the information includes minimizing the error phrases; alternatively, one other paradigm that maximizes the probability of the parameter estimates within the distribution serves the identical objective equally nicely or better. Comparison of Bayes, Least-Squares, SteadyState, and Chiou Methods For theophylline dosing, the Bayes method and others, including the traditional steady-state methodology, had been in contrast by Hurley and McNeil (1988). The steady-state technique was additionally useful, however none of the strategies was sufficiently accurate, in all probability due to other variables, corresponding to saturation kinetics or using an inappropriate compartment mannequin. Model becoming in pharmacokinetics typically involves the search for a set of parameters that fits the info, a scenario analogous to discovering a degree within a large geometric area. The Bayesian strategy uses prior data, and, in essence, guides the search pointer to a proximity within the geometric area where the estimates usually have a tendency to be discovered (reducing variability however rising subjectivity). Many algorithms use some form of gradient- or derivative-based methodology; different algorithms use a variable sequential simplex methodology. Some common pharmacokinetic algorithms for parameter estimation are (1) Newton�Raphson with first and second derivatives, (2) Gauss�Newton methodology, (3) Levenberg�Marquardt technique, and (4) Nelder�Mead simplex methodology. As discussed in relation to the mixed-effect models in later sections, assuming a relationship similar to ClR proportional to Clcr (technically called linearization) reduces the minimum variety of data essential for parameter estimation. Traditional pharmacokinetic parameter estimation may be very accurate, supplied that sufficient samples can be taken for the person patient. The drawback is that only a few comparatively homogeneous wholesome topics are included in pharmacokinetic studies, from which dosing in different patients have to be projected. In the medical setting, sufferers are usually much less homogeneous; patients range in intercourse, age, and body weight; they could have concomitant disease and may be receiving a number of drug remedies. Even the food plan, life-style, ethnicity, and geographic location can differ from a particular group of "regular" subjects. However, the important data needed about the pharmacokinetics of medication in sufferers at different levels of their disease with various therapies can solely be obtained from the identical population, or from a collection of pooled blood samples. The advantages of inhabitants pharmacokinetic evaluation using pooled knowledge were reviewed by Sheiner and Ludden (1992) and included a abstract of population pharmacokinetics for dozens of drugs. Pharmacokinetic analysis of pooled knowledge of plasma drug focus from a big group of topics may reveal a lot information about the disposition of a drug in a population. Unlike information from a person topic collected over time, inter- and intrasubject variations have to be considered. Both pharmacokinetic and nonpharmacokinetic factors, corresponding to age, weight, intercourse, and creatinine focus, ought to be examined in the model to decide the relevance to the estimation of pharmacokinetic parameters. In addition, to pharmacokinetic parameters, many examples of population plasma data have been analyzed to determine inhabitants factors. Multiplicative coefficients or parameters for patient factors can also be estimated. The mannequin may test for other fastened effects on the drug as a end result of factors such as age, weight, and creatinine clearance. The model describes the noticed plasma drug focus (Ci) by method of a model with: 1. Pk = mounted effect parameters, which embody pharmacokinetic parameters or patient factor parameters. For example, P1 is Cl, P2 is the multiplicative coefficient including creatinine issue, and P3 is the multiplicative coefficient for weight. Random impact parameters, including (a) the variance of the structural (kinetic) parameter, Pk, or intersubject variability throughout the popu2 lation, k; and (b) the residual intrasubject variance or variance due to measurement errors, fluctuations in individual parameter values, and all other errors not accounted for by the other parameters. There are usually two dependable and practical approaches to inhabitants pharmacokinetic information evaluation. The estimates from all topics are then mixed to obtain an estimate of the parameters for the population. This technique attempts to match the data and partition the unpredictable variations between theoretical and observed values into random error terms. For example, in the instance cited by Beal and Sheiner (1985), 116 plasma concentrations were collected from 39 patients with various weight, age, gender, serum creatinine, and congestive heart failure situations. With a lot of factors and solely limited information, and with hidden components presumably affecting the pharmacokinetics of the drug, the evaluation might sometimes be misleading. Beal and Sheiner (1985) suggested that the primary concomitant issue should be measured every time possible. Several examples of population pharmacokinetic information analysis using clinical information are listed beneath. Many medicine have been analyzed with inhabitants pharmacokinetics to yield the information not obtainable using the traditional two-stage technique (Sheiner and Ludden, 1992). One example involving analysis of population plasma concentration information concerned the drug procainamide. The drug clearance of a person in a 722 Chapter 22 group may be assumed to be affected by several factors (Whiting et al, 1986). These factors embody physique weight, creatinine clearance, and a clearance issue P1 described within the following equation: Cldrug j = P1 + P2 (Ccreatinine j) + P3 (weight j) + Clj (22. Proper sampling can yield valuable information about the distribution of pharmacokinetic parameters in a inhabitants. Pooled scientific drug concentrations taken from hospital patients are generally not well managed and are much tougher to analyze. A mixedeffect mannequin can yield useful details about numerous demographic and pathophysiologic components that may affect drug disposition in the affected person population. The Akaike Information Criterion and the Schwarz Criterion lead to selection of essentially the most acceptable model more typically than does the F check, which tends to choose the simpler model even when the extra advanced model is informative. Clearance was quite robust among the many completely different methods and usually properly estimated. Other pharmacokinetic parameters are extra delicate to model choice, significantly the obvious elimination fee fixed.
Buy generic skelaxin on lineWhile the radiosurgery-alone remedy arm had worse native and distant management rates muscle relaxant cephalon cheap generic skelaxin uk, subsequent salvage remedy appeared to be effective (Chang et al. Therefore, in chosen patients, the radiosurgery-only approach could be appropriate as preliminary therapy. Size, number, and site of the lesions in addition to patient-specific elements together with performance standing, comorbidities, and the extent of extracranial disease need to be taken under consideration by the treating physician when evaluating a affected person for either surgical procedure or a radiosurgical approach. Surgery Surgical removal of mind metastases has been consistently shown to profit patients with melanoma mind metastases (Staudt et al. Surgery offers the benefits of confirming the analysis, immediate relief of mass effect, and enchancment of neurological signs. However, the majority of sufferers with mind metastases handled with surgical procedure do eventually progress and succumb to disease. Patients with a single brain metastasis and people with a metastasis in the supratentorial area had extended survival times. Of notice, some patients survive a few years after surgical procedure; these are probably to be sufferers with single mind lesions and without extracranial illness (Sampson et al. Patients with multiple resected mind metastases (n = 15) had shorter survival than the patients who underwent resection of a single lesion (n = seventy six, median 5. Although postoperative mortality is generally low, one might argue that this is due to number of patients with higher extracranial tumor control and better efficiency status that had been chosen for surgery. Retrospective information show that if full surgical resection of all lesions is achieved, then sufferers with a number of mind lesions, like these with a single lesion solely, can derive benefit from surgery. But perhaps the biggest evolution in the surgical administration of those patients is the shift away from the prior commonplace of care of surgical resection followed by whole-brain radiation. The native recurrence fee dropped to 20% with combinatorial therapy (Patchell et al. Furthermore, subsequent studies were unable to substantiate the advantage of whole-brain radiation in publish resected sufferers (Armstrong et al. Since then, surgical methods have developed to extra regularly respect oncological principals of resection with a margin, if possible, that reduces the native recurrence rate to 20% (Yoo et al. The declining use of whole-brain radiation as an immediate follow-up to surgical resection was additional accelerated by the related cognitive issues described for whole-brain radiation and because of the truth that as soon as the option of whole-brain radiation has been used, this potential treatment modality has been eliminated from the therapeutic portfolio. Systemic Therapies for Melanoma Brain Metastases Responses to systemic chemotherapy regimens have historically been very discouraging for patients with brain metastases in multiple cancers, including melanoma Table 19. The first agent used to deal with brain metastases sufferers with melanoma was dacarbazine, which was also the primary chemotherapeutic agent to acquire approval for the remedy of metastatic melanoma. Owing to the restricted bioavailability of the drug in the cerebrospinal fluid, nevertheless, response charges within the mind have been low (Anderson et al. However, it achieves intracranial response rates of only 10%, similar to the low response rate seen in sufferers with extracranial disease solely (Agarwala et al. Sorafenib, a multityrosine kinase inhibitor, additionally has been evaluated in multiple trials of patients with melanoma. In most of them, sorafenib was combined with other agents, and patients had been included within the trial if their mind metastases were secure or asymptomatic (Agarwala et al. Ipilimumab + (2012) fotemustine Long (2012) Dabrafenib (patients with out previous local therapy for mind metastases: 74 with V600E mutation; 15 with V600K mutation) 89 fifty two (43�63) Dabrafenib (patients with 83 earlier local remedy for brain metastases: sixty five with V600E mutation; 18 with V600K mutation) Rompoti et al. Immunotherapy-based regimens have been used for many years in the treatment of metastatic melanoma. High-dose interleukin-2 is related to a low rate of responses and can trigger vital poisonous results but in addition can induce long-term responses in a small subset of patients. In an analysis of 274 patients with melanoma who obtained high-dose interleukin-2, 20 had brain metastases. This result instructed that the presence of brain metastases was the most significant predictor of an absence of clinical response to interleukin-2. In addition, one has to contemplate the risk of elevated intracranial pressure in patients who receive this remedy. Interleukin-2 has also been studied in the context of biochemotherapy regimens for melanoma patients. In such regimens, interleukin-2 is given as a continuous infusion, and is mixed with both interferon and multiagent chemotherapy. One study of 20 sufferers found that the outcomes of a biochemotherapy have been related in patients with and with out mind metastases if the mind metastases were controlled with multidisciplinary treatment. Ipilimumab was approved for the remedy of patients with metastatic melanoma in 2011. Notably, the overall antitumor exercise, 2-year survival rate, and security in this examine had been much like what has been reported in melanoma patients with out brain metastases who were treated with ipilimumab (Margolin et al. Another creator reported a mind management fee of 16% and a response price of 8% in 38 sufferers with melanoma brain metastases who were handled with ipilimumab as a part of the prolonged entry program (Konstantinou et al. Adding fotemustine to ipilimumab might further enhance clinical profit (Di Giacomo et al. While the outcomes with, and approval of, ipilimumab symbolize a breakthrough in melanoma, latest outcomes counsel that other immunotherapies could additionally be even more helpful. Two of the sufferers who experienced a complete response in the mind for six months ultimately developed diseases at new websites in the mind in addition to at extracranial websites. Six of the seven sufferers with full responses within the mind achieved an total partial response. Combining Radiation with Systemic Therapy Combining whole-brain radiation with chemotherapy or immunotherapy has been one other topic of investigation. The elements offered listed right here are all retrospectively collected, and some studies included patients treated over 5 a long time in the past. There stays a critical unmet want for brand spanking new therapies and medical trials for sufferers with melanoma mind metastasis. The a quantity of recent laboratory and medical advances on this disease help that rational and more effective therapies could also be developed in the close to future. This opportunity is matched by the challenge of figuring out factors that can allow for appropriate stratification and analysis of those trials, and in the end for personalized remedy choice for patients. While this challenge is massive, the quickly advancing remedy landscape for this disease helps that such efforts have tremendous promise and potential to meaningfully influence survival in the close to future for patients with this extremely aggressive disease. Malignant melanoma and central nervous system metastases: incidence, analysis, therapy and survival. A nomogram for predicting distant mind failure in patients treated with gamma knife stereotactic radiosurgery without entire brain radiotherapy. Systemic remedy for unresectable metastatic melanoma: impact of biochemotherapy on long-term survival. Predictive elements for the development of mind metastasis in advanced unresectable metastatic melanoma.
Buy online skelaxinA retrospective medical report evaluate examine confirmed that serum creatinine concentration is an insufficient screening take a look at for renal failure in older patients in addition to it leads to spasms pregnant belly skelaxin 400 mg low cost underinvestigation and underrecognition of renal failure within the older population (Swedko et al, 2003). Drugs that are eradicated primarily by way of glomerular filtration, including aminoglycoside antibiotics, lithium, and digoxin, have an elimination clearance that decreases with age in parallel with the decline in measured or calculated creatinine clearance (Ljungberg and Nilsson-Ehle, 1987; Cusack et al, 1979; Sproule et al, 2000). The renal clearance of drugs present process lively renal tubular secretion also decreases with growing older. For instance, the decrease in renal tubular secretion of cimetidine parallels the lower in creatinine clearance in older sufferers (Drayer et al, 1982). Conversely, the ratios of renal drug clearance/creatinine clearance of both procainamide and N-acetylprocainamide decrease within the older patients, suggesting that with getting older the renal tubular secretion of these drugs declines more quickly than creatinine clearance (Reidenberg et al, 1980). The Baltimore Longitudinal Study of Aging followed 254 healthy volunteers for up to 25 years and prospectively discovered that creatinine clearance by way of 24-hour urine assortment decreased zero. However, one-third of these individuals had no decrease in creatinine clearance in about 20 years. Later research showed that getting older itself might have a minor impact on kidney operate but the confounding factors similar to hypertension and continual heart diseases account for the decline of kidney perform (Fliser et al, 1997a, 1997b). The current Italian Longitudinal Study on Aging also confirmed that the age-related discount of kidney perform was associated with coexisting cardiovascular ailments and different threat components (Baggio et al, 2005). Age-Related Changes in Transporters Transporters similar to P-glycoprotein, organic anion transporting peptide, natural cation transporter, and natural anion transporter involve in drug absorption, Application of Pharmacokinetics to Specific Populations: Geriatric, Obese, and Pediatric Patients 743 distribution, metabolism, and excretion (see Chapters eleven and 12). However, very few revealed data exist for the impact of growing older on the expression and function of drug transporters. The comparatively few printed articles up to now supplied conflicting results on the impact of advancing age on P-glycoprotein activity and expression (Mangoni, 2007). However, a positron emission tomography research showed that older members have significantly decreased P-glycoprotein function within the inside capsule and corona radiata white matter and in orbitofrontal areas, which can partly clarify the vulnerability of aging mind to white matter degeneration (Bartels et al, 2009). Anyhow, longitudinal pharmacodynamic studies that measure individual charges of growing older for the specified variable are uncommon. The following are examples to illustrate the impact of getting older on the pharmacodynamics of specific therapeutic areas. For more complete listings, the readers can check with other revealed articles (Bowie and Slattum, 2007; Trifir� and Spina, 2011; Corsonello et al, 2010). Effects of Age on Pharmacodynamics in Older Adults Age-related pharmacokinetic modifications are usually properly characterized as mentioned above. This may be partly as a result of the comparatively simpler bioanalytical methods that contain figuring out drug concentrations in serial samples of biomaterial versus the challenge to develop and validate acceptable measures of drug responses. Majority of knowledge for the age-related variations in human pharmacodynamics originate from cross-sectional studies. Cross-sectional research assume that the mean differences observed between age groups replicate the change that occurs in study individuals with the passage of time with out directly observing the identical individuals in longitudinal research. This assumption may be invalid because of the following (Bowie and Slattum, 2007; Trifir� and Spina, 2011): � Difficulties to differentiate chronological age versus biological age or physiological effects versus pathological effects � Selective mortality results since the oldest study cohort contains only those participants who Drugs That Act on the Central Nervous Systems Benzodiazepines. Changes in pharmacodynamics rather than pharmacokinetics with growing age could be more related to explain the altered response to benzodiazepines. The precise mechanisms responsible for the increased sensitivity to benzodiazepines with growing older are unknown. Diazepam, flurazepam, flunitrazepam, nitraze, midazolam, and triazolam present age-related enhance in sensitivity to cognitive and sedative effects of benzodiazepines within the absence of significant pharmacokinetic modifications (Swift et al, 1985; Castleden et al, 1977; Greenblatt et al, 1981, 2004; Kanto et al, 1981; Albrecht et al, 1999). A reduced response to both agonist and antagonist of cardiac 1 and bronchial 2 receptors is observable (Vestal et al, 1979; Scott et al, 1995). Beta-adrenoreceptors are coupled with Gs proteins, which in flip are linked to adenylate cyclase. Age-associated decreases in Gs activity are observed in vitro from human heart beta receptors (White et al, 1994). A downregulation of beta-adrenergic receptors can also explain the upper systemic drug concentration essential with increasing age to reach the specified effect (Scarpace et al, 1991). The risk�benefit ratio for the treatment of beta receptor antagonists wants careful analysis because greater doses may be more practical however with safety concerns (Dobre et al, 2007). Evidence exists of a larger inhibition of synthesis of vitamin K-dependent clotting elements at similar plasma warfarin concentrations in older sufferers than young sufferers. However, the precise mechanism of this age-related change in sensitivity is unknown. Age is among the strongest predictors of the anticoagulant effects of warfarin (Miao et al, 2007; Schwartz, 2007). Confounders of Pharmacokinetics and Pharmacodynamics in Older Adults Factors corresponding to pharmacogenetic polymorphisms, nutrition, concomitant drugs, smoking, and ingesting habits can affect the disposition and motion of medication in older sufferers. Another confounding issue for drug disposition and motion in older sufferers could be frailty (Shi and Klotz, 2011; Sitar, 2012). Wynne reported that frailty might impair conjugation pathways (sulfation and glucuronidation) for metoclopramide (Wynne et al, 1993). Nevertheless, frailty is related to larger inflammatory markers corresponding to C-reactive protein, interleukin-6, or tumor necrosis factor-alpha (Fried et al, 2009; Clegg et al, 2013). The perform of various neurotransmitters in dopaminergic, serotonergic, and cholinergic systems could also be influenced not solely by the getting older process itself but in addition by the psychopathology of psychiatric issues, including schizophrenia, depression, or dementia (Meltzer, 1999). Thus, the results of psychotropic medication within the older patients may differ between sufferers with and with out these psychological diseases. In common, the interindividual pharmacokinetic variability is prominent, which is often due not only to the influence of age-related physiological adjustments but additionally to the impression of comorbidities and drug interactions (Shi and Klotz, 2011). Mallet et al suggest a multiprofessional staff method to manage drug interactions and optimize drug therapy in older sufferers (Mallet et al, 2007). The advanced interactions amongst comorbidity, polypharmacy, modifications in pharmacodynamic sensitivity, and comparatively modest pharmacokinetic changes in the older patients warrant the dosing advice to observe the standard wisdom of "start low and go sluggish" (Schwartz and Abernethy, 2009; Shi and Klotz, 2011). Emerging Approaches to Avoid Adverse Drug Eventsin Older Adults the Beers record (also generally known as Beers criteria) has been extensively used as a reference for pharmacists and physicians in the United States to enhance using treatment in older patients. Beers, advocated the use of specific criteria developed through consensus panels for identifying inappropriate use of medicines in older patients. Application of Pharmacokinetics to Specific Populations: Geriatric, Obese, and Pediatric Patients 745 the Beers listing was originally developed for frail older individuals living in nursing properties. Subsequently, it was updated and expanded to embrace new medical conditions and generalized to the older population regardless of their frailty status or place of residence. The present Beers listing is the fourth rendition after revision of the 1991, 1997, and 2003 editions (The American Geriatrics Society 2012 Beers Criteria Update Expert Panel, 2012). The Europeans additionally compiled an inventory that guides the prevention of inappropriate use of medications in older patients (Laroche et al, 2007). These anticholinergic results have been linked with cognitive impairment in older sufferers (Cancelli et al, 2008). Drugs with sedative opposed effects are also of concern for older patients since these sedative results could cause falls and bone fractures (Leipzig et al, 1999; Ensrud et al, 2002), which can further cause older sufferers to lose independence. The anticholinergic risk scale method ranks medicines for anticholinergic potential on a 3-point scale (0, no or low threat; three, excessive anticholinergic potential).
References - Luisi SV, Ashraf MH, Gula G, et al: Anomalous origin of the right coronary artery with aortopulmonary window: functional and surgical considerations, Thorax 35:446-448, 1980.
- Imai T, Kubo T, Watanabe H. Chronic gastritis in Japanese with reference to high incidence of gastric carcinoma. J Natl Cancer Inst 1971;47:179.
- Levin B, Mackay HMM, Oberholzer VG. Argininosuccinic aciduria, an inborn error of amino acid metabolism. Arch Dis Child 1961;36:622.
- Newton HB, Ruda R, Soffietti R. Neuronal and mixed neuronal-glial tumors. In: Grisold W, Soffietti R (eds) Handbook of Clinical Neurology, Neuro- Oncology. Amsterdam: Elsevier/Academic Press, 2012; 551-567.
- Rubin MA, Bismar TA, Andren O, et al: Decreased alpha-methylacyl CoA racemase expression in localized prostate cancer is associated with an increased rate of biochemical recurrence and cancer-specific death, Cancer Epidemiol Biomarkers Prev 14:1424n1432, 2005.
- Aaronson KD, Patel H, Pagani FD. Patient selection for left ventricular assist device therapy. Ann Thorac Surg. 2003;75(Suppl):S29-S35.
- Holland R, van Haelst UJ. Mammary carcinoma with osteoclast-like giant cells. Additional observations on six cases. Cancer. 1984;53(9):1963-1973.
|