|
Dr Agnieszka Crerar-Gilbert - Consultant in Cardiothoracic Intensive Care &
- Anaesthesia
- St George�s Cardiothoracic Intensive Care Unit
- London
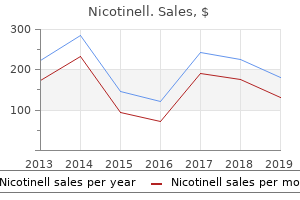
Nicotinell dosages: 52.5 mg, 35 mg, 17.5 mg
Nicotinell packs: 1 packs, 2 packs, 3 packs, 4 packs, 5 packs, 6 packs, 7 packs, 8 packs, 9 packs, 10 packs

Order nicotinell with a mastercardConvergence of major afferent neurones also can clarify the phenomenon of referred ache quit smoking chantix cheap nicotinell 17.5mg otc, where pain seems to come from structures other than the injured or infected tissue. These interneurones can have an inhibitory effect both by decreasing the discharge of the excitatory transmitter (a process called presynaptic inhibition), or by inhibiting the second-order neurone (a process referred to as postsynaptic inhibition). The activation of the interneurones is caused by impulses from bigger afferent nerves from the identical neural section of the body because the nociceptor, corresponding to A mechanoreceptor neurones, which are stimulated by touch or by impulses descending from greater centres of the brain in a course of known as descending inhibition. This gate management mechanism most probably can happen in any respect synaptic levels of the pain pathway. This is when there is a rise in activity (facilitation), leading to a rise within the energy and/or the length of the ensuing ache. Wind-up is due to repetitive activation of nociceptive C fibres, which brings about an enhanced response to subsequent activity in these fibres. It is caused by an elevated release of substance P from the presynaptic neurone or by the enhanced response of postsynaptic receptor websites for substance P and glutamate. Nociceptor pathways From the subnucleus caudalis, axons from the second-order nociceptor neurones cross the midline and project by way of the trigeminothalamic tract to the ventrobasal nuclei of the contralateral thalamus. The neurones which are believed to be involved with emotion and motor responses to nociception project to the posterior and medial teams of thalamic nuclei either instantly or via intermediate synapses in the reticular formation. Dental ache the stimuli that trigger pain when applied to intact enamel include electrical currents and intense heating or cooling applied to the enamel. The stimuli that trigger dental ache when applied to uncovered dentine and/or pulp are far more varied and include, not solely electrical current, heating and cooling, but additionally mechanical probing, drying, application of hypertonic options, hydrostatic strain and, in pulp only, the appliance of algogenic chemical substances. Stimuli that trigger pain when applied to human dentine have been proven to improve fluid movement via dentine both by increasing fluid flow outwards from the pulp or by producing inward fluid circulate in path of the pulp. It would appear that intradental nerves are extra easily excited by fluid flow outwards from the pulp than inwards in the direction of the pulp. These substances are all excitatory but their influence could be modulated by an inhibitory management mechanism often referred to as gate management. The basic principle behind the gate management principle of ache is that the signals transmitted through the pathways from firstto second-order neurones should cross via a so-called gate, managed by small adjacent cells (interneurones): these are either inhibited (closing the gate) or excited (opening the gate). In this fashion, the gate is fully closed, and therefore no pain is felt, or totally open, during which case the ache would be extreme. In most instances the pain would probably fall 172 Age-related changes probably act immediately on the nerves within the inside dentine or pulp. It is assumed that transient pain arising from dentinal stimulation is mediated by A and A myelinated fibres when nerve endings have been activated through the hydrodynamic mechanism, as the results are localized and the ache persists for the size of time the stimulus is utilized. In the case of continual pulpal inflammation and the place the stimulus persists for hours, there are apparent changes in the haemodynamics of the pulp and in nerve excitability that can be attributed to the discharge of algogenic chemical substances in the pulp. It is assumed that these chemicals stimulate pulpal afferent, unmyelinated C fibres and provides rise to the persistent, less properly localized, sluggish ache characteristic of nociceptor C fibre activation. These could also be localized as discrete pulp stones both singly or in small teams, or be diffusely scattered all through the pulp. Age-related adjustments A number of age-related changes are seen in the pulp: � It will get smaller with age, as secondary dentine deposition continues throughout life. On a moist weight basis, dentine accommodates 70% inorganic materials, 20% organic materials and 10% water. The mature dentinal tubule incorporates an odontoblast process that passes from the pulp�dentine border to the enamel�dentine junction. In demineralized sections, predentine stains in one other way from the remainder of the (mineralized) dentine matrix. Collagen fibrils within the circumpulpal dentine are oriented parallel to the dentinal tubules. The granular layer (of Tomes) on the cement�dentine border is an impact produced by terminal dilatations and branching of dentinal tubules. A dead tract occurs when the dentinal tubules in that region turn out to be utterly obliterated by peritubular dentine. Reparative dentine closely resembles secondary dentine with an everyday tubular structure. Dentine sialoprotein is post-transcriptionally cleaved from the same gene product as dentine phosphophorin. An incremental line reflecting a diurnal rhythm of dentine secretion during improvement 2. A structural feature which could be present separating major and secondary dentine 174 Thirteen: Dental tissues. This is a floor part of outer dentine within the crown, a piece of the enamel�dentine junction (A) being seen. Lumsden) A B this micrograph is of a floor part of the root of a tooth immersed in water. Identify the horizontally disposed strains arrowed, indicating their approximate distance aside. How would you account for the truth that a carious lesion reaching the enamel�dentine junction in a 175 Thirteen: Dental tissues. List the three main hypotheses proposed to explain dentine sensitivity, indicating arguments for and towards each one. This is a micrograph of a longitudinal section of the crown of a tooth mounted in Canada balsam. Thus, dentine has extra inorganic materials than bone or dental cementum, however less than dental enamel. This is expounded to the truth that the organic matrix of enamel is largely eliminated throughout development, whereas collagen in dentine remains behind. Primary curvatures are broad, sinuous curvatures of the dentinal tubules produced by the odontoblasts as they migrate inwards and become crowded during dentinogenesis. There continues to be controversy concerning the extent of the odontoblast processes inside the dentinal tubules. This relates mainly to the difficult technical drawback of fixing and preserving the very lengthy, delicate course of in the tubule. Ultrastructural proof suggests that cell processes progressively withdraw from the peripheral dentine. The collagen fibrils in circumpulpal dentine are oriented perpendicular to the long axis of the tubules. A relationship also exists between the quantity of peritubular dentine formed and the degree of attrition. Where regions between adjoining calcospherites fail to mineralize, hypomineralized interglobular dentine is seen. The presence of sensory intratubular axons has been confirmed by research involving axonal transport of radioactive amino acids injected initially into the trigeminal ganglion. They are extra quite a few over the cusps or incisal edges of teeth, and little evident in root dentine. The granular layer has additionally been related to the presence of minute interglobular areas produced as a end result of incomplete mineralization. Von Ebner strains are short-period traces that replicate the presence of a diurnal rhythm. They seem perpendicular to the lengthy axis of the dentinal tubule and are about 3 m aside.
Purchase nicotinell 52.5mg amexAirway Obstruction Obstruction of the respiratory airways is in plenty of circumstances a medical emergency quit smoking devices nicotinell 35 mg discount. The location of the airway obstruction might vary anatomically and may be supraglottic, laryngeal, tracheal or bronchial. A mixture of anatomical airway segments is often involved, as in the presence of a tumour resulting in tracheobronchial obstruction. It may be related to tracheal or laryngeal obstructions, as within the presence of anaphylaxis with resultant vocal twine oedema. Complete higher airway obstruction results in speedy respiratory embarrassment and moreover presents with dyspnoea, tachypnoea, diaphoresis (excessive sweating) and a subsequent lack of consciousness. There is also use of the accent respiratory muscle tissue (the belly and intercostal muscles) as an effort is made to re-establish the conventional intrathoracic pressures. Examination of the thorax reveals deep retractions of the intercostal muscles, Clubbing this refers to the thickening of the distal aspect of the finger with a rise within the convex form of the nail bed. It is related to cigarette smoking and is related to a number of cardiopulmonary pathologies including lung cancer, lung abscess, pulmonary fibrosis, persistent obstructive pulmonary illness, emphysema, pleural and mediastinal malignancies, cystic fibrosis and lung abscess. Examination of the Chest the chest ought to be examined with the affected person in each the supine and upright positions. This allows both the anterior and posterior chest in addition to the symmetry to be evaluated. Associate scoliosis is seen in up to 20 per cent of sufferers with pectus excavatum, which is a congenital sternal depression or concavity related to the distal third of the sternum. Conversely, pectus carinatum is a outward bulge or convex deformity of the sternum. A failure of expansion of one facet of the chest throughout a respiratory cycle signifies the presence of underlying pathology. The chest circumference can be measured on the level of the nipples during each the inspiratory and expiratory phases. Counting the Ribs � the ribs can be counted utilizing fastened landmarks on the rib cage: � the sternal notch may be felt on the superiormost side of the manubrium. Auscultation the lung ought to be examined by auscultation anteriorly and posteriorly as nicely as at multiple levels to evaluate all the lobes. The breath sounds heard over the normal lung parenchyma are softer and more even than these heard over the trachea and larynx, as the airway sounds are tempered by the chest wall and regular lung parenchyma. Inspiratory breath sounds are heard all through the inspiratory section of respiration, while regular expiratory breath sounds are heard only in the course of the first half to two-thirds of the expiratory cycle. The expiratory section of respiration throughout normal air flow is usually twice as long as the inspiratory section. This regular sample on auscultation of the breath sounds is termed vesicular breath sounds. Instead, auscultation is performed medial to the medial borders of the scapula within the auscultatory triangle. Auscultation of the lung within the upright position could reveal the presence of an effusion and might present useful data on the level and volume of such an effusion. The breath sounds are difficult to auscultate or are diminished when the lung parenchyma not is in apposition to the chest wall, stopping the optimal conduction of the breath sounds. The underlying pathology consists of pneumothorax, hydrothorax, haemothorax, chylothorax, pleural thickening, empyema and atelectasis. Obese sufferers with elevated quantities of subcutaneous tissue may also present a challenge when auscultating the breath sounds. Bronchial breath sounds are appreciated when the lung parenchyma becomes consolidated and the auscultatory qualities of the breath sounds heard in the principle airway and over the consolidated parenchyma turn into related. Wheezes are coarse, high-pitched breath sounds that might be current during both the inspiratory and expiratory phases of the respiratory cycle. They suggest bronchiectasis or narrowing of the airway and are current in reactive airway ailments such as asthma. Crackles are breath sounds that the majority intently resemble the sound made by screwing up a sheet of paper. They range in coarseness, and are uniformly present in sufferers with pulmonary oedema. They symbolize the sound made by the opening and shutting of the distal airways that are surrounded by diseased parenchyma. Crackles may be alternated with rales, but these terms are sometimes used to discuss with the same auscultatory discovering. Pleural rubs are present in irritation of the pleural surfaces and are due to the visceral and parietal pleura sliding over each other. A reddish vascular-appearing mass on the chest wall in a patient who has had prior chest wall irradiation could represent an angiosarcoma. A pulsatile mass in the supraclavicular fossa may be indicative of a post-obstructive aneurysm in the setting of thoracic outlet syndrome involving the axillary artery. Anteriorly, there are incomplete C-shaped cartilaginous rings, whereas posteriorly the trachea is membranous. Placing a finger in the suprasternal notch and palpating the placement of those rings can verify its place in the midline. Tension pneumothoraces, mediastinal tumours, cervical lots or quantity loss from a hemithorax could result in tracheal deviation. Auscultation of the chest might provide a clue as to the underlying pathology when tracheal deviation is current. For instance, a lack of breath sounds in a hemithorax along side tracheal deviation is suggestive of a pressure pneumothorax. Percussion Percussion of the chest is normally performed on the posterior facet of the thoracic cavity within the interspaces between the ribs. Consolidation of the underlying lung parenchyma, hydrothorax, haemothorax, chylothorax and lung- or pleural-based plenty result in decreased resonance or dullness to percussion. Hyperresonance is related to pneumothoraces or air-trapping in the related lung segments. As the examination of the proper hemithorax proceeds caudally, dullness to percussion is experienced within the region of the liver. Palpation Palpation of the chest wall might reveal sternal fractures, rib fractures, the presence of pathological lymphadenopathy or plenty. Bony or cartilaginous tumours can be appreciated by palpating the surface of the chest wall and costochondral joints, in addition to the sternum. Supraclavicular lymphadenopathy may be indicative of malignancies of the lung or breast. Similarly, axillary lymphadenopathy could also be current in breast cancer or different infectious pulmonary pathologies.
Syndromes - Inherited metabolic disorders such as familial hypercholesterolemia
- Painful menstruation
- A family history of neuromuscular disease
- During puberty: 0.3 - 10.0 mIU/ml
- Separated sutures
- Hairy cell leukemia
- Miscarriage
- CT scan angiography (using contrast dye)
- After-surgery exercise and instructions are not followed.
- Sit or lay in different positions to keep your joints from becoming stiff
Order nicotinell master cardThis creates an osmotic gradient and interstitial fluid flows into junctional and sulcular epithelium and sulcus quit smoking quit key purchase 52.5mg nicotinell fast delivery. Flow fee can additionally be immediately affected by: � elimination of the fluid by the lymphatic system of the gingival tissues � the filtration coefficient of the junctional and sulcular epithelia � variations in oncotic stress of the interstitial fluid and sulcular fluid. Within the lamina propria, the collagen fibres are organized as a community to enable free motion, and the elastin fibres permit recoil to prevent the mucosa being chewed. The lips, cheeks, alveolus, flooring of the mouth, ventral surface of the tongue and taste bud have a lining mucosa. There is a free group of the junctional and sulcular epithelium, which serves to enhance fluid circulate from the capillaries into the connective tissues as a consequence of the host response. The production of an inflammatory exudate allows the passage of cells and enormous proteins into the Lip the lip has skin on its outer floor and labial mucosa on its internal floor. The lips have striated muscular tissues in their core that are a part of the muscle tissue of facial expression. Substantial amounts of minor mucous salivary glands are present in the submucosa beneath the oral mucosa. The central core of lamina propria has smaller, secondary papillae branching from it. The filiform papillae have an abrasive function throughout mastication when the bolus is compressed towards the palate. The connective tissue papillae of the lamina propria are comparatively long and slender, and comprise capillary loops. The proximity of these vessels to the floor, mixed with the translucency of the epithelium, provides the floor a purple look - hence its name. The junctional region between the vermilion zone and the oral mucosa is called the intermediate zone. The vermilion zone has a unique transitional phenotype with options of each epidermal and oral mucosal epithelium. Fungiform papillae Fungiform papillae are found as isolated, mushroomshaped papillae scattered between the filiform papillae. They are covered by a relatively thin epithelium that will or is in all probability not keratinized, and have a vascular core of lamina propria. Foliate papillae Foliate papillae may be current as one or two longitudinal clefts at the aspect of the posterior part of the tongue. Circumvallate papillae Circumvallate papillae are the biggest papillae and are surrounded by a trench-like feature. Groups of mucous glands are also seen throughout the muscle of the tongue, significantly in the posterior half. Ventral floor of the tongue the ventral floor of the tongue and the ground of the mouth are covered by typical lining mucosa. The submucosa is extensive on the ground of the mouth however indistinct (if not absent) on the ventral floor of the tongue, the place the mucosa binds right down to the tongue muscles. The thinness of the epithelium and the vascularity of the connective tissue make this a route by which some medication can quickly reach the bloodstream. Taste buds Taste buds are situated within the epithelium around the partitions of the circumvallate papillae, but are also present in small numbers on the fungiform and foliate papillae, on the soft palate and on the epiglottis. Two kinds of cell are current in the style bud: the supporting cell and the taste cell. Specialized mucosa the anterior two-thirds of the dorsum of the tongue may be considered a specialized gustatory mucosa because of the presence of style buds and papillae. Dorsal surface of the tongue An vague groove, the sulcus terminalis, divides the dorsal surface of the tongue into an anterior two-thirds (palatal surface) and a posterior third (pharyngeal surface). The anterior two-thirds of the tongue is roofed with numerous papillae, specifically filiform, fungiform, foliate and circumvallate. Lingual tonsil A collection of lymphoid follicles lies on the posterior third of the tongue, which is roofed by a lining mucosa. The follicles are deep crypts lined with epithelium and containing a mass of lymphoid material. The gingiva forms a attribute interdental col between teeth which are spaced. The sulcular epithelium is unique in having both an internal and an external basement membrane (basal lamina). The vermilion (red) zone on the lip is keratinized, with pronounced dermal papillae. Like different lining epithelium, junctional epithelium accommodates cytokeratins 4 and thirteen. Trans-septal fibres move from the cementum of adjacent tooth above the alveolar crest. The turnover time of masticatory epithelium is generally quicker than that for lining epithelium. Turnover time for collagen within the gingiva is just like that within the periodontal ligament. In this demineralized part the place the damaged vertical line (arrowed) represents the acquired pellicle: a. Identify the structures labelled A�C in this electron micrograph of a keratinocyte from one of the layers of the oral epithelium. Name the non-keratinocytes present within the oral cavity, describing their origin, morphology and performance. How is the function of the oral surface of the exhausting palate related to its operate Parakeratosis is generally present in the masticatory mucosa of the gingival and palate. An interdental col only happens between cheek enamel which are in contact and shall be lined by a non-keratinized epithelium. When tooth are spaced, the col will disappear and be replaced by a keratinized epithelium. The junctional epithelium possesses two basal laminae; the internal basal lamina is found at the interface with the tooth floor, the external basal lamina on the interface with the underlying connective tissue. Together with the underlying blood vessels, this provides the vermilion zone its pink coloration. Junctional epithelium accommodates easier cytokeratins, such as cytokeratin 19, perhaps reflecting its derivation from odontogenic epithelium. These fibres present an anatomical basis whereby all the tooth in the arch are linked together. Turnover time for the hard palate is of the order of about 3�4 weeks, whereas that for buccal mucosa is nearer 2 weeks. The turnover time of gingival collagen is about three times slower than that of the periodontal ligament. The presence of a basal lamina on its exterior and internal surfaces makes this epithelium unique. Due to the presence of cytokeratins, Merkel cells can be recognized by immunohistochemical techniques using antibodies for cytokeratins 8/18 and 20.
Cheap nicotinell 17.5 mg on lineOsteoblasts secrete the organic matrix of bone that initially is represented by an unmineralized layer quit smoking years ago generic nicotinell 52.5mg otc, the osteoid. Useful markers of the osteoblast phenotype include osteocalcin and osteoblast transcription issue, Runx2 (Cbfa-1). Alkaline phosphatase exercise, though not completely specific to bone, can also be a reliable indicator of osteoblastic differentiation. At the surface of alveolar bone adjacent to the periodontal ligament, extrinsic Sharpey fibres cross kind of perpendicularly into the osteoid layer. In addition to secreting the formative elements of bone, the osteoblast secretes molecules controlling its own activity (such as growth factors, cytokines and prostaglandins) and that of the osteoclast. Osteoclasts Osteoclasts are derived from fusion of haemopoietic cells of the macrophage/monocyte lineage, giving rise to multinucleated cells. A useful marker for osteoclasts is the enzyme tartrate-resistant acid phosphatase. Characteristically, human osteoclasts could additionally be up to one hundred m in diameter and have on common 10�20 nuclei. When actively resorbing, osteoclasts possess a ruffled border composed of many tightly packed microvilli adjacent to the bone surface, offering a large surface area for the resorptive process. Here, the plasma membrane is smooth and the organelle-free cytoplasm beneath it incorporates numerous contractile actin microfilaments (surrounded by two vinculin rings). The sealing zone serves to connect the cell very carefully to the floor of bone, mainly due to the presence of cell membrane adhesion proteins generally known as integrins. However, in contrast with osteoblasts, they present a considerable reduction within the intracellular organelles associated with protein synthesis. They are housed in lacunae, possess quite a few cell processes that run in channels (canaliculi) within bone, and 223 Sixteen: Alveolar bone: construction and composition able to degrading the organic matrix of bone. There is thus a clear relationship between bone deposition and bone resorption, and this relationship is mediated biochemically. These bone-bound bioactive growth elements are activated by subsequent osteoclastic bone resorption and bind to their receptors on osteoblasts and osteoclasts, influencing bone remodelling. As a discount in the mechanical loads impinging on bone is related to bone loss, it could be assumed that such loading is generally required to stimulate the modelling/remodelling processes of bone necessary to maintain normal bone structure. Strains need to be intermittent (rather than continuous), and the osteogenic response is dependent upon the scale of the load and the frequency and rate of software. To preserve bone mass may only require the applying of comparatively few loading cycles. The molecular mechanisms whereby forces impinging on the bone are transduced into bone resorption or deposition remain elusive, though many theories have been proposed. Osteocytes, together with the floor layer of osteoblasts/bone-lining cells, seem to be the obvious candidates for detecting strain inside bone. Deformation of bone following loading is thought to deform the cell processes/cell membranes both directly, or indirectly through movement of tissue fluid residing in the lacunocanalicular system. These changes finally lead to the manufacturing and launch of molecules that initiate an osteogenic response. Sharpey fibres Extrinsic Sharpey fibres inserting into the cribriform plate are derived from the principal fibres of the periodontal ligament. Sharpey fibres are significantly distinguished within the cervical portion (alveolar crest region) of the alveolar bone. Here, where bone is compact, Sharpey fibres might penetrate the bone to a considerable depth. Sharpey fibres entering alveolar bone are much less quite a few but thicker than those at the cementum surface. Because of the attachments of numerous bundles of collagen fibres, the cribriform plate has additionally been known as bundle bone. These traces are outstanding in bundle bone on the distal floor of the socket wall during physiological mesial drift of the enamel. Bone will also include reversal strains, representing the positioning of change from bone resorption to bone deposition. Resorption and deposition of bone There is shut correlation between resorption and deposition of bone. This has led to the concept that the osteoblast has a controlling influence in the development and maturation of the osteoclast. Clearly, there must be tight management to guarantee a balance between the two processes, as any disruption of this steadiness can lead to metabolic bone disease (such as osteopetrosis and osteoporosis). From a resting state, the sequence of remodelling consists of 4 main phases: � Resorption: recruitment, migration and activation of osteoclasts, inflicting bone resorption. The site becomes occupied by 224 Resorption and deposition of bone Osteoblast formation Osteoblast formation is initiated from pluripotent mesenchymal stem cells. These cells give rise to intermediate progenitor cells that type osteoprogenitors (immature and mature forms) and pre-osteoblasts. It takes about eight cell divisions before an osteoblast finally differentiates to form an osteoid seam that mineralizes to produce bone. Among the earliest markers to point out that a stem cell is progressing along an osteogenic phenotype is the expression of the nuclear transcription issue, core binding factor 1 (Cbfa1, also known as Runx2). This is liable for regulating the production of a selection of important protein merchandise in bone matrix. Following the resorptive section, osteoclasts are thought to be eliminated by apoptosis. Two further essential factors concerned within the activation of osteoclasts are acidification and hypoxia. Sixteen Osteoclast formation Osteoclast formation differs from the other cells associated with bone. In the incisor area, little cancellous bone is current between internal and outer cortical plates of alveolar bone. In the alveolar crest area, Sharpey fibres may extend completely via the alveolar bone. The main receptors for parathormone (which results in bone resorption) are discovered on osteoblasts. Osteoclasts, like periodontal fibroblasts, degrade collagen in intracellular collagen profiles. Mesial drift of a molar tooth is accompanied by deposition of bone mesially and resorption of bone distally. The nuclei current in osteoclasts are derived from a single cell that undergoes numerous divisions. The canaliculi of osteocytes in alveolar bone are preferentially orientated in the course of the periodontal ligament.

Purchase nicotinell 52.5 mgThe possible mechanisms within the periodontal ligament/ follicle liable for eruption should be elucidated and quit smoking quit now purchase nicotinell 17.5 mg with visa, particularly there ought to be a short description of the possible roles of the periodontal fibroblasts and/or of periodontal vascular/tissue hydrostatic pressures. The final paragraph of the essay should indicate that eruption is also multifactorial in terms of the process of eruption. Furthermore, the tissues must transform to sustain eruptive movements and, importantly, the quantity (and rate) of eruption relies upon the forces of eruption exceeding forces resisting eruption. They: � produce the organic matrix that becomes mineralized � management the transport of calcium ions into the matrix � determine the presence and distribution of particular matrix parts (proteoglycans and glycoproteins) that regulate the method. The basic mechanisms for mineralization are matrix vesicle-mediated mineralization and heterogenous mineralization or epitaxy. Overview Mineralization of organic tissue is both strictly regulated and distinctive to every mineralized tissue. The mechanisms of mineralization of bone and dentine share close similarities whereby an unmineralized matrix, osteoid or predentine, is calcified by a mixture of matrix vesicle-mediated mineralization and heterogenous mineralization. However, for all three tissues, a selection of tissue-specific proteins and proteoglycans tightly regulate mineralization by inhibiting mineralization processes or by guiding mineral deposition. Such proteins, and the cells that synthesize them, are subsequently essential in controlling the rate of mineralization, allowing ordered progress of the mineral crystals and stopping premature crystal fusion. To acquire hydroxyapatite, we should first precipitate a less steady, simpler calcium phosphate known as brushite and then rework this into hydroxyapatite. This first mineral in mantle dentine, early bone and calcified cartilage is provided by matrix vesicles. These vesicles present a controlled micro-environment to concentrate calcium and phosphate, within the presence of a variety of enzymes (including alkaline phosphatase). Mineral crystals develop within the vesicles and eventually burst out and become associated with the natural collagenous matrix of predentine or osteoid. As matrix vesicles are the one crystalline constructions present in the first-formed dentine (mantle dentine) and bone, Learning aims You should: � know the mechanisms regarding matrix vesicle-mediated mineralization and perceive the idea of heterogenous nucleation (epitaxy) as related to mineralization of bone and dentine natural matrix � understand the similarities with and differences from the mineralization of enamel � perceive the role of bone- and dentine-specific proteins in inhibiting or selling mineralization. When contemplating the basic ideas of mineralization of bone and dentine it turns into clear that mineralization is a controversial topic. Mineral crystal formation entails two stages: � Firstly, nucleation or the formation of small embryo crystals � Secondly, crystal development, which is characterised by the deposition of calcium and phosphate onto the crystal surface. Osteopontin is a phosphorylated protein capable of selling mineralization, and osteonectin has been shown to inhibit development of hydroxyapatite crystals while selling the binding of calcium and phosphate to collagen. Although particular glycoproteins and proteoglycans have been proven to have differing roles in promoting and inhibiting mineralization and crystal growth (including the presence of dermatan sulphate proteoglycans in predentine), other elements are additionally necessary in regulating mineralization. Pyrophosphate is found in gentle tissues and body fluids and actively inhibits mineralization. In exhausting tissues, pyrophosphatase could be recognized and degrades any pyrophosphate current, allowing mineralization to happen. Heterogenous nucleation In heterogenous nucleation, crystal growth is induced by the provision of a second, stable part on which a crystal lattice may be formed. Crystal progress is better promoted on crystalline materials having related lattice spacings, an idea often recognized as epitaxy. In the context of mineralizing tissues, the prime candidate is the natural matrix. After mantle dentine has been synthesized and secreted, and odontoblast differentiation is complete, the odontoblasts express the matrix components required for nucleation websites and the preliminary hydroxyapatite crystal seeds develop on the expense of calcium and phosphate that move into the matrix via the cell. Mineralization of circumpulpal dentine Investigations into the mineralization of circumpulpal dentine have advised that odontoblasts actively transport calcium ions to the mineralization website via lively transport by way of the cell. Deposition of calcium occurs on to a template formed by type I collagen, and mineral crystal deposition happens at the gap zone inside the collagen fibrils. This dentinespecific protein is secreted at the mineralizing front and is highly phosphorylated and highly acidic, thus having a excessive affinity for calcium and hydroxyapatite surfaces. Changes within the conformation of the protein enable it to bind rising numbers of calcium ions. Several other proteins have been proven in vitro to be associated with mineralization. Initial mineralization of root dentine It is price noting two options the place there are variations between the mineralization of coronal dentine and that of root dentine. These concern the first-formed root dentine, which is called the hyaline layer: � the primary considerations the secretion into this layer from the adjoining epithelial root sheath cells of the enamelrelated protein ameloblastin. Whether this protein is associated with differentiation of cells or with mineralization awaits clarification. The subsequent extension of mineralization outwards is believed to permit for higher bonding of the cementum and dentine (see page 137). Mineralization of bone Mineralization of bone has sturdy similarities with that of dentine in that the initial process is governed by matrix vesicle-mediated mineralization, with matrix vesicles 136 Mineralization of cementum budding off from the plasma membrane of the osteoblast, followed by heterogenous nucleation. Calcium and phosphate ions required for mineralization are derived from the plasma. As with the mineralization of predentine, mineralization of osteoid requires remodelling of the original tissue matrix to remove inhibitory proteoglycans. The presence of different tissue-specific proteins such as osteopontin, osteocalcin and bone sialoprotein additional influences the mineralization in a similar method to that seen in dentine mineralization. These nanospheres can work together with other elements and should type an organizing construction. For example, they bind tightly to enamel crystals via the C terminal part of the molecule, which is cleaved off soon after secretion. This is the key to understanding how the amelogenin nanospheres regulate hydroxyapatite crystal progress. The amelogenin nanospheres control growth by appearing as spacers between the crystals, providing space for model new crystal deposition and inhibiting uncontrolled mineralization. They achieve this by selling development in the C axis (length of the crystal) and forestall premature crystal�crystal fusion. It is that this mechanism that explains the unusually long initial enamel crystal appearance. In the maturation phase of amelogenesis, the matrix proteins have a lowered function to play, as most organic materials has been degraded and lost, and the matrix proteins are removed lengthy before crystal growth ends. Eleven Mineralization of enamel the mechanism of mineralization of enamel differs from that seen in the mesenchymally derived hard tissues bone and dentine. No matrix vesicles are current, so the only mechanism is heterogenous nucleation/epitaxy and the seeding of a mineral crystal on the organic matrix. However, the presence of enamel-specific proteins, amelogenins and non-amelogenins. During enamel maturation, amelogenins are broken down, allowing crystal growth and hard tissue formation. Non-amelogenin proteins Concerning the non-amelogenin proteins, enamelin is assumed to act as a nucleation web site, as it has been advised that it might work together with the crystallites. The position in mineralization of the opposite non-amelogenin proteins, tuftelin and ameloblastin, is still open for debate, although ameloblastin could also be involved as a outcome of its localization to the prism boundary region. Whether underlying dentine crystallites type the seeding mechanism or whether that is totally regulated by the natural matrix of cementum awaits clarification.
Nicotinell 17.5 mg mastercardFibroadenomas Fibroadenomas are benign tumours of the breast which are frequent in women of their late teens to their early 30s quit smoking 7 weeks ago generic nicotinell 52.5 mg visa. Most fibroadenomas grow to 1�2 cm in diameter, and their size can fluctuate as a outcome of the affect of hormones through the menstrual cycle. If the triple check is according to a fibroadenoma, the lesion could be managed conservatively with a follow-up examination in 6 months. There is often a characteristic oil cyst (a collection of lipids surrounded by a membrane) on mammography in the area of trauma, leading to the diagnosis of fats necrosis; nonetheless, the realm of trauma might reveal fibrosis and calcifications that may mimic malignancy on mammography. Galactoceles these are milk-filled fluid collections most commonly seen during lactation or after the cessation of lactation. Galactoceles routinely current as a slightly tender mass and could be a number of or bilateral. Most galactoceles resolve after aspiration, and if the patient is asymptomatic the galactocele can be merely noticed. If the pores and skin is necrotic, surgical incision and drainage is warranted to drain the purulent fluid. It is necessary to keep in thoughts that management of a subareolar abscess is simply a temporizing measure as most of those sufferers will need definitive therapy that requires surgical elimination of the diseased ducts. Trauma After trauma to the breast, a lady could develop fats necrosis, which is the result of saponification of the adipose tissue. Gynaecomastia is most often seen in infancy, during puberty and after the age of fifty. Although bodily ache can be associated with gynaecomastia, most males present for analysis as a end result of the psychological stress the condition can cause. The listing of causes of gynaecomastia is intensive and should be evaluated while taking a detailed historical past from the affected person. The breast examination is carried out whereas the affected person is within the supine place with his arms behind his head. The two fingers are then brought collectively and the tissue behind the nipple is palpated. Patients with gynaecomastia have bilateral concentric, disk-like tissue that can typically really feel rubbery. Mammography and/or ultrasound has additionally been employed in patients with gynaecomastia to additional delineate whether or not an underlying malignancy is present. Male breast most cancers accounts for about 1 per cent of all instances of breast most cancers. Fixation to the pores and skin or to the underlying muscle can also be appreciated on bodily examination. As in ladies with a suspected breast malignancy, men must bear the triple check, which includes a detailed historical past and physical examination, mammography and/or ultrasound, and tissue analysis with a core needle biopsy. A mastectomy with a sentinel lymph node biopsy is the popular methodology of surgical remedy, as the relatively small quantity of breast tissue in a person limits the utilization of breast conservation remedy. They are used as screening modalities in girls with an extremely excessive risk of breast cancer or during the search for an occult breast major, mostly one which has introduced with enlarged axillary nodes. The transducer may be positioned immediately over the lump or area of tenderness, and careful scanning of the underlying area can confirm or exclude the presence of a mass. While there are ultrasound traits which are kind of suggestive of malignancy, the safest course is to undertake tissue sampling for anything not definitively shown to be a cyst. Percutaneous biopsies may be carried out on the bedside, cost less and are less invasive than open surgical biopsies. Breast cancer could additionally be treated by lumpectomy (removal of the tumour with a rim of surrounding tissue) followed by radiation therapy, or by mastectomy. Further therapy with chemotherapy or hormone-blocking brokers is commonly employed. Women who present with large or locally advanced breast cancer are generally treated with chemotherapy first; surgery is then carried out after the tumour has shrunk. Radiation therapy is used after lumpectomy to lower the chance of local recurrence. A very complete set of guidelines is on the market from the National Comprehensive Cancer Network and could also be accessed from their website after free registration as a medical skilled. Reconstructive surgery could also be mixed with mastectomy or carried out at a later time. Autologous tissue reconstruction methods contain tissue flaps or transfers, and essentially the most commonly utilized techniques embody the transverse rectus abdominis myocutaneous flap and the latissimus dorsi myocutaneous flap. Most patients who endure prosthetic reconstruction have tissue expanders positioned on the time of the mastectomy that are sequentially expanded over the next few weeks after which eventually changed with a permanent implant. Key Points Fine Needle Aspiration Cytology Fine needle aspiration is a quick and cheap biopsy that can be carried out at the bedside underneath ultrasound steerage. Fine needle aspiration can also decide whether a breast mass is strong or cystic, and aspiration of a breast cyst may be not solely diagnostic, but additionally therapeutic. After a small incision has been made in the pores and skin with a scalpel, a disposable, spring-loaded hand-held system with a 12�18 gauge needle is used to obtain a minimum of three tissue samples from the lesion of concern. Common symptoms of breast issues might include a mass or lump, ache and nipple discharge. A detailed history should include a dialogue of the presenting downside, any earlier breast problems, an in depth gynaecological history and a household history. The bodily examination includes a detailed inspection and palpation of the breasts and axilla, with the patient in each the sitting and supine positions. Benign breast disease is a typical entity in ladies aged 20�40 and covers a large spectrum of situations. Gynaecomastia is the results of an imbalance within the oestrogen/ androgen ratio that favours increased circulating oestrogen, and the list of its causes is in depth. Male breast most cancers accounts for roughly 1 per cent of all breast cancer circumstances. Breast cancer may be handled with lumpectomy, mastectomy, radiation, chemotherapy and/or hormonal blocking brokers. Compared with women, males with breast most cancers: a On common present at an earlier age b Stage for stage have the identical prognosis as girls with breast cancer c Are typically hormone receptor-negative d Account for 10 per cent of all breast cancers Answer c Genetic testing. Men have a reported average age at analysis from their late 60s to early 70s, which is roughly 10 years older than in ladies. It is extra generally undertaken when a patient is suspected of having distant (metastatic) illness or recurrent breast most cancers. For every of the following descriptions, select the more than likely matches for the presentations given below. Each choice may be used as quickly as, greater than once or under no circumstances: 1 Simple cyst 2 Fibroadenoma 3 Fat necrosis four Galactocele 5 Mammary fistula 6 Gynaecomastia 7 Subareolar abscess a Often results from trauma to the breast and may be confused with breast cancer on imaging b Most commonly seen during lactation and is the outcome of ductal obstruction Answers a 3 Fat necrosis. After trauma to the breast, a lady could develop fats necrosis, which is the results of saponification of the adipose tissue. The main problem with fats necrosis is that it could be confused with breast most cancers on imaging.
Weidenrinde (Willow Bark). Nicotinell. - Osteoarthritis ("wear and tear arthritis"), rheumatoid arthritis, weight loss when taken in combination with other herbs, treating fever, joint pain, and headaches.
- Treating low back pain.
- Dosing considerations for Willow Bark.
- How does Willow Bark work?
- What other names is Willow Bark known by?
- Are there any interactions with medications?
- Are there safety concerns?
- What is Willow Bark?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96918
Generic nicotinell 35mg fast deliveryWinging of the scapula may be tested whereas the arm is lifted forwards or when the patient pushes the outstretched arm against a wall quit smoking 6 month benefits cheap nicotinell 17.5 mg line. Preganglionic accidents additionally current with early neuropathic ache secondary to nerve root avulsion. Once the placement of the damage in relation to the dorsal root ganglion has been decided, an effort should be made to decide whether the damage entails the upper or decrease brachial plexus. Classification Common aetiology Description Neurapraxia Nerve compression Local myelin harm, nerve intact Axonotmesis Nerve crush Axonal interruption with intact Schwann cells Neurotmesis Nerve transection Axonal interruption with disrupted surrounding connective tissues Table 9. This leads to paralysis of the deltoid, biceps, rhomboid, brachioradialis, supinator, supraspinatus and infraspinatus muscular tissues. Patients typically current with the arm hanging by their aspect and medially rotated, with the forearm prolonged and pronated. This presents with a characteristic claw hand as a outcome of a lack of operate of the ulnar nerve and subsequent weak spot of small muscle tissue of the hand, as nicely as weak point of the flexors of the wrist and fingers. It presents with painful dysaesthesias in the distribution of the palmar aspect of the first three digits, typically wakening the patient at night time. There may be Median Nerve the median nerve has contributions from the C5�T1 nerve roots. It then crosses to the medial facet of the artery on the degree of coracobrachialis. It provides all the forearm flexor muscles aside from flexor carpi ulnaris and a part of flexor digitorum profundus. The cutaneous provide of the median nerve covers the thumb and radial two and a half fingers anteriorly and posteriorly as far proximally as the center phalanx. The median nerve is prone to entrapment or damage at particular sites alongside its path. Next, on the forearm stage, the nerve may be entrapped by certainly one of two structures: the bicipital aponeurosis or the pronator teres muscle. When the nerve is entrapped at either of these sites, sufferers present with clinical signs of injury to the main trunk of the median nerve. A third web site of damage lies deep within the forearm, the place the anterior interosseous nerve, a motor branch of the median nerve, can be damaged. The posterior interosseous nerve gives off branches to the supinator, extensor carpi ulnaris, extensor digitorum communis, extensor digiti minimi, abductor pollicis longus, extensor pollicis longus and brevis, and extensor indicis muscular tissues. Ulnar Nerve the ulnar nerve is a direct continuation of the medial wire of the brachial plexus; it has contributions from the C7, C8 and T1 nerve roots. It then enters the forearm, passing through the two heads of the flexor carpi ulnaris, and runs along the ulna. It also offers rise to a palmar and a dorsal sensory branch that innervate the little finger and the ulnar facet of the ring finger. In the hand, it provides the hypothenar muscle tissue (flexor, abductor and opponens digiti mimimi), adductor pollicis brevis and all the dorsal and palmar interossei. Injury or entrapment of the ulnar nerve on the elbow usually occurs secondary to trauma or a fracture of the lateral epicondyle of the humerus. Entrapment of the ulnar nerve at the elbow can be idiopathic or arise secondary to arthritis; this situation is recognized as cubital tunnel syndrome. Patients with an ulnar nerve harm at this degree typically current with pain and discomfort within the ulnar nerve distribution (the internal border of the hand and the fourth and fifth digits), with intrinsic hand muscle weak spot. This deformity is clear when making an attempt to lengthen the fingers (unlike the deformity secondary to a median nerve damage, which happens while attempting to make a fist). Motor deficits because of ulnar nerve injuries at the degree of the wrist are similar to these encountered in accidents to the nerve on the stage of the elbow. Sensory deficits in patients with ulnar nerve accidents on the stage of the wrist sometimes spare the dorsal facet of the hand, since the dorsal cutaneous branch of the ulnar nerve originates in the forearm and is normally preserved. In the arm, the radial nerve innervates brachioradialis and extensor carpi radialis longus and brevis. Lumbosacral Plexus 181 the cutaneous innervations of the radial nerve include the posterior cutaneous nerve of the arm (which originates in the axilla), the inferior lateral cutaneous nerve of the arm (which originates in the arm), the posterior cutaneous nerve of the forearm (which originates within the forearm) and the superficial department of the radial nerve, which provides roughly two-thirds of the dorsum of the hand. This may result from direct compression by a lesion, entrapment on the arcade of Frohse or strenuous muscle exercise. This is as a end result of of preservation of the wrist extensors (extensor carpi radialis longus and brevis). Unlike a posterior cord harm within the brachial plexus, a radial nerve harm exhibits intact axillary nerve and thoracodorsal nerve innervations. This plexus varieties over the sacroiliac joint and nearly immediately leaves the pelvis by way of the greater sciatic foramen. Its main branches � the gluteal nerve, the sciatic nerve and the posterior femoral cutaneous nerve of the thigh � then lie directly behind the hip joint. Musculocutaneous Nerve the musculocutaneous nerve arises from the lateral wire of the brachial plexus. It passes via the coracobrachialis muscle after which enters the arm between the brachialis and biceps brachii. It supplies sensory innervation to the forearm by way of the lateral cutaneous department of the forearm. The musculocutaneous nerve can be injured via stretching, for instance after shoulder dislocation, or it might be entrapped between the heads of the biceps. Since the nerve innervates the coracobrachialis, brachialis and biceps brachii muscle tissue, harm causes weak point in elbow flexion and supination of the forearm, with a depressed biceps reflex. Axillary Nerve the axillary nerve is a department of the posterior twine of the brachial plexus and carries nerve fibres from the C5 and C6 nerve roots. It supplies sensory innervation to the lateral facet of the arm via the lateral cutaneous department of the arm. Compression of the axilla by crutches or by a fracture of the surgical neck of the humerus can also injury the axillary nerve. Injury leads to a flat shoulder deformity as a outcome of paralysis of the deltoid and teres minor muscle tissue. The initial 15� of arm abduction is preserved because the initiation of abduction is a perform of the supraspinatus muscle. Patients with an axillary nerve injury additionally present with a sensory disturbance over the lateral aspect of the upper arm. It reaches the thigh by skirting around the pelvic brim, coming into the thigh under the lateral a half of the inguinal ligament. The solely signs of illness in this nerve, that are often identified as meralgia paraesthetica, are painful paraesthesias � uncomfortable burning, tingling sensations in the anterolateral side of the thigh. The symptoms are brought on by entrapment or stretching of the nerve under the lateral facet of the inguinal ligament. The illness is widespread in people who are gaining or reducing weight, or throughout or after pregnancy. The symptoms are sometimes associated to solely a single posture, similar to sitting or standing. Examination reveals hyperaesthesia, or not often hypoaesthesia, in the anterior lateral thigh.
Discount nicotinell 17.5 mg fast deliveryHyperparathyroidism presents with symptoms of hypercalcaemia with out gland enlargement quit smoking nhs best nicotinell 52.5mg. Which one of many following statements is true of the association between a lingual thyroid and cervical athyrosis All of the following are true except: a Nephrolithiasis is commonly associated with hyperparathyroidism b Parathyroid adenoma is the most typical explanation for hyperparathyroidism c Cataract occurs in hypoparathyroidism whereas band keratopathy is seen in hypercalcaemia d Parathyroid carcinoma is associated with hypoparathyroidism Answer c Physiological modifications. Physiological adjustments corresponding to puberty and pregnancy cause a diffuse enlargement known as a simple goitre. Lingual thyroid is associated with cervical athyrosis in about 70 per cent of instances. This reply is unfaithful as parathyroid carcinoma causes hypercalcaemia secondary to hyperparathyroidism. On examination, the swelling is within the midline and moves with deglutition in addition to tongue protrusion. Ultrasound scanning suggests a 2 cm cystic swelling below the hyoid bone and above the thyroid, with a normal thyroid gland. A thyroglossal cyst occurs within the path of embryological descent, presents in younger age groups and moves with protrusion of the tongue. Breast complaints are widespread and in the overwhelming majority of cases are as a outcome of benign alternations within the regular physiology. The difficulty for the clinician lies in distinguishing those relatively few girls in whom underlying malignancy is the cause. There are in fact different breast conditions that require analysis and remedy, however in these cases too the prudent clinician will first exclude carcinoma. Men have a small quantity of breast tissue which will hypertrophy and require therapy. This chapter first evaluations the overall conduct of the breast-directed historical past and bodily examination after which briefly discusses particular widespread diagnoses. Women can also be referred for breast examination when a routine screening mammogram has shown an abnormality or because of a strong family historical past of breast cancer. Thus, for the girl presenting with a breast lump, enquire how she first famous it and whether or not the lump has grown or modified along with her menstrual cycles. Typically, breast cancers both develop or stay unchanged throughout a interval of observation, whereas benign breast lumps wax and wane with hormonal influences. Pain and tenderness are more widespread with benign issues but are also seen with breast most cancers. Pay attention to any earlier historical past of breast issues; particularly, confirm whether the girl has had a biopsy. Ask the age of menarche, number of pregnancies, age at first pregnancy and whether or not the woman continues to be having durations. In common, breast nodularity and tenderness related to fibrocystic modifications shall be maximal between ovulation and menstruation; subsequently Table 28. It is necessary to know if the girl is presently taking oral contraceptives or postmenopausal hormone therapy, and whether or not she has taken these up to now. Finally, a personal historical past of most cancers of the contralateral breast or other websites is necessary. Ovarian and endometrial carcinoma are each associated with an elevated threat of breast cancer. Some malignancies can really metastasize to the breast but this is rare and is normally associated with other manifestations of systemic spread. A cellular examining lamp offers additional illumination when examining the nipples for discharge or when looking for refined indicators of skin retraction. A cape or other drape that might be elevated to reveal the breasts supplies some warmth and comfort till the examination begins. The breasts change during development and development, and enlarge significantly throughout being pregnant. This kind exhibits how a clinician has recorded the placement, size and physical traits of a breast lump. Then have her put her palms on her hips and push in to tense her pectoralis main muscular tissues. The superficial phlebitis is self-limiting and often resolves inside a few weeks. Sharma, Department of Radiation Oncology, All India Institute of Medical Sciences. Smears could also be made for cytological examination but this rarely yields helpful information. While the girl remains to be sitting up with her palms on her hips, feel the axillae for lumps. Small cellular nodes are sometimes felt bilaterally in slender young ladies however the presence of unilateral enlarged nodes suggests underlying malignancy. Discharge Bright purple blood Causes the most common cause is a benign intraductal papilloma. Similarly, really feel the supraclavicular fossae for nodes, generally an indication of more advanced malignancy. Nodes lying posteriorly round serratus anterior and latissimus dorsi, and the lateral group around the neck and shaft of the humerus, may most simply be felt with the examiner standing behind the lady. If no lump is palpable within the ipsilateral breast, extra imaging research (see below) should be carried out. Always consider other causes of isolated axillary adenopathy, corresponding to melanoma (examine the arm and trunk for pigmented pores and skin lesions) and lymphoma (check for enlarged nodes in different regions). If the breasts are involuted and pendulous, feel the feel and thickness of each breasts by grasping every breast between the thumb and fingers. Diffuse and extensive involvement of the breast with lobular carcinoma is sometimes most simply found on this manner as the tumour might not type a discrete mass but somewhat exchange a large amount of breast tissue in an insidious trend. Repeat this examination with three ranges of pressure � light, medium and agency � in order that nothing is missed. Begin by getting a basic sense for the feel and degree of nodularity of the unaffected breast parenchyma. If an abnormality is found, notice the size, location (typically by clock face orientation and distance from nipple or areolar border), mobility and associated characteristics (Table 28. If the presenting complaint is breast ache or tenderness, search not solely breast lumps, but additionally different causes for pain in the area. Any lump or space of tenderness must be further examined by imaging research (see below) and freely employing the triple test cited above. While the girl is mendacity supine, finish your examination by palpating the liver for metastatic deposits. Other indicators of metastatic illness embody localized skeletal pain and tenderness, and pleural effusion.
Generic nicotinell 17.5mgDuring the seventh week of intrauterine life quit smoking 6 months ago how should i feel nicotinell 17.5 mg low price, a centre of ossification appears on this fibrous tissue at a site close to the long run psychological foramen. From this centre, bone formation spreads rapidly backwards, forwards and upwards, around the inferior alveolar nerve and its terminal branches (the incisive and psychological nerves). However, the 2 plates of bone stay separated by fibrous tissue to kind the mandibular symphysis. At a later stage in the growth of the physique of the mandible, continued bone formation markedly will increase the dimensions of the mandible, with improvement of the alveolar process occurring to encompass the growing tooth germs. The sphenomandibular ligament ossifies at its websites of attachment to type the lingula of the mandible and the spine of the sphenoid bone. As the creating tooth germs attain the bell stages (see page 114), creating bone turns into closely associated to it to type the alveolus. With the onset of root formation, inter-radicular bone develops in multirooted enamel. Further growth of the ramus is related to a backward unfold of ossification from the body and by the looks of secondary cartilages. Between the tenth and fourteenth weeks in utero, three secondary cartilages develop throughout the rising mandible. The largest, and most necessary, of those is the condylar cartilage, which, as its name suggests, seems beneath the fibrous articular layer of the longer term condyle. By proliferation and subsequent ossification, the cartilage is assumed by some to function an necessary centre of development for the mandible, functioning up to in regards to the twentieth 12 months of life. Less essential, transitory, secondary cartilages are seen associated with the coronoid course of and within the region of the mandibular symphysis. Postnatally, the ratio of body to ramus is bigger at birth than within the grownup, indicating a proportional increase with time within the growth of the ramus. Ossification of the symphysis is full in the course of the second year, the 2 halves of the mandible uniting to type a single bone. There is some evidence that the angle of the mandible decreases from delivery to maturity. In basic terms, increase within the top of the physique happens primarily by formation of alveolar bone, although some bone can additionally be deposited alongside the decrease border of the mandible. Increase in the length of the mandible is completed by bone deposition on the posterior floor of the ramus with compensatory resorption on its anterior surface, accompanied by deposition of bone on the posterior surface of the coronoid course of and resorption on the anterior floor of the condyle. Increase in width of the mandible is produced by deposition of bone on the outer surface of the mandible and resorption on the inner floor. Present evidence means that proliferation of the condylar cartilage is a response to development and not its cause. The behaviour of these matrices primarily determines the expansion of each skeletal unit. For example, the coronoid course of types a skeletal unit acted upon by the temporalis muscle. Sectioning of the temporalis muscle during early mandibular growth might result in atrophy or full absence of a coronoid course of in the adult mandible. Similarly, the alveolar course of is influenced by the teeth, the condyle by the lateral pterygoid muscle, the ramus by the medial pterygoid and masseter muscle tissue, and the physique by the neurovascular bundle. The centre of ossification appears through the eighth week of intrauterine life, near the site of the developing deciduous canine tooth. From the region of the creating deciduous canine, ossification spreads throughout the developing maxilla into its rising processes (palatine, zygomatic, frontal and alveolar processes). At one time it was thought that the incisor-bearing a part of the maxilla, which develops from the frontonasal course of (see page 101), had a separate centre of ossification. Among the brokers that present the forces separating the maxilla from the adjoining bones (thus permitting development on the sutures) are the rising eyeballs, cartilaginous nasal septum and orbital pad of fat. It has been suggested that the rising nasal septum pulls the maxilla ahead by means of a septopremaxillary ligament that runs from the anterior border of the nasal septum posteroinferiorly towards the anterior nasal spine and intermaxillary suture. As within the lower jaw, growth in top of the maxilla is expounded to the event of the alveolar process. The maxillary sinus seems as an out-pocketing of the mucosa of the middle meatus of the nose initially of the fourth month of intrauterine life. Forward progress of the whole face (including the maxillae) depends upon progress of the spheno-occipital synchondrosis on the base of the skull. The predominant activity in the fundus of the socket is considered one of bone resorption, except for teeth whose eruptive pathway is bigger than the length of the basis. On events the place bone deposition is seen lining the alveolus, it may be related to relocation of the erupting tooth inside the growing jaws. Sharpey fibres from the periodontal ligament become connected to the wall of the alveolus during tooth eruption, though the timing is expounded to whether or not the tooth is of the deciduous or permanent dentition (see page 210). The bone of the alveolar wall could then be referred to as bundle bone (see page 222). Development of the tongue the anterior two-thirds of the tongue develop from three swellings: the two lateral lingual swellings (buds) and the midline median lingual bud (tuberculum impar). Each is formed by proliferation of mesenchyme beneath the endodermal lining of the first pharyngeal (branchial) arch. The posterior third of the tongue develops from a single midline swelling, the hypopharyngeal eminence, which is derived primarily from the third pharyngeal arch with a small contribution from the 4th arch. The eminence overgrows the 2nd arch (the copula) to merge with the 1st arch swellings. The various embryological origin of the tongue explains its various sensory supply: � General sensation to the anterior two-thirds of the tongue is provided by the lingual nerve, a nerve of the first pharyngeal arch. The muscular tissues of the tongue develop primarily from occipital somites that migrate into the growing tongue carrying their nerve supply, the hypoglossal nerve, with them. Thus, in a fibrocellular condensation, a centre of ossification appears during which osteoblasts lay down first-formed or woven bone. As the tooth develop, bone extends from the developing mandible and maxillae to encompass and protect the enamel, forming the alveolus. The alveolus is separated from the growing enamel organ by the dental follicle. Later, the teeth turn out to be separated from each other by the development of interdental septa. As in different sites, the collagen fibres within the newly formed alveolar bone have a more variable diameter and lack a preferential orientation, giving the bone a matted (basket weave) look when considered in polarized gentle. This immature bone, termed woven bone, has larger and extra numerous osteocytes compared with grownup bone. The source of the cells forming alveolar bone is unsure, though some have instructed that it may be from neural crest cells of the investing layer of the dental follicle (see web page 116). During crown formation, relocation of the tooth germ throughout the growing jaws may be related to acceptable patterns of resorption and deposition on the interior surfaces of the alveolar bone. With the onset of tooth eruption, the bone overlying the tooth undergoes resorption to present a pathway of eruption (see web page 118). In Development of the thyroid gland this gland develops between the median lingual bud and the hypopharyngeal eminence.
Buy nicotinell 52.5 mg on lineThe contents of the vesicles (secretory granules) are discharged into the extracellular space at the distal finish of the cell towards the surface of the first-formed dentine quit smoking zap buy 52.5 mg nicotinell free shipping. Almost as soon as the enamel matrix is launched extracellularly, the preliminary calcium hydroxyapatite crystallites seem within it as skinny, needle-like crystallites. As the ameloblasts migrate outwards (centrifugally), small processes from the odontoblasts might get caught up between them. When the early enamel starts to mineralize round them, these processes will turn into entrapped as enamel spindles. Incremental markings Periodic changes within the nature or orientation of the enamel crystallites or enamel matrix or enamel prisms produce short-period or long-period incremental markings. A diurnal rhythm produces a daily cross-striation across every prism roughly 4 m aside, while approximately every 7 days (range 6�10), an enamel stria (of Retzius) is produced outlining the mineralizing front and working obliquely to the surface. These striae end on the floor of the enamel as perikymata, except for the first-formed striae overlying the cusps of the tooth. In teeth mineralizing before delivery, an exaggerated stria, the neonatal line, is current representing the enamel fashioned during the general disturbance in metabolism occurring over the few days following delivery. As the ameloblasts continue to move away from the dentine surface, a cone-shaped process (Tomes process) quickly forms at the distal, secretory end of the ameloblasts. When that is thought of in three dimensions, it could be seen that four ameloblasts contribute to each enamel prism and that every ameloblast contributes to 4 prisms. Additional cell contacts are current between ameloblasts and cells of the stratum intermedium. Enamel maturation is carried out by the same ameloblast cells that secreted the primary matrix, but in a very changed kind. The interval throughout which the ameloblasts change from a secretory to a maturation form is the transition stage. The variety of ameloblasts is reduced by as much as 50% by apoptosis (programmed cell death). In those ameloblasts that remain, the organelles related to protein synthesis. The quantity of stellate reticulum is reduced in order that blood vessels invaginating the exterior enamel epithelium come to lie near the proximal finish (base) of the ameloblasts. Newly formed enamel consists of about 65% water, 20% natural material and 15% calcium hydroxyapatite crystallites by weight. The stage during which enamel modifications from its lightly calcified and organic-rich state into its ultimate extremely mineralized and organic poor state is termed the maturation stage. During maturation, enamel crystallites increase in width and thickness at the expense of water and organic matrix. Calcium and phosphate ions transfer through the ameloblasts and into the maturing enamel, while water and degraded enamel proteins pass in the other way. During this process, the common thickness of the crystallites increases from about 1. The degradation of the enamel matrix, most likely by serine proteases released from the enamel organ, appears to precede mineral acquire. Indeed, on the initial stage of maturation, the house brought on by matrix loss is occupied by water, with the enamel turning into extra porous. To replicate the change in perform from the secretory stage to the maturation stage, the ameloblasts undergo morphological changes. Having a decreased peak and a great reduction within the quantity of organelles associated with protein synthesis, the distal finish of the cell exhibits numerous infoldings, forming a striated border. This morphology alternates with that of the smooth-ended ameloblast, by which the striated border is absent. Modulation between the 2 types appears to occur between 5 and 7 times throughout maturation. This modulation may indicate alternation between resorptive phases, throughout which water and organic components are removed, and secretory phases, when mineral ions are added to the maturing enamel. Maturation takes a substantial time frame and, like enamel formation, proceeds from the information of the cusps down in path of the cervical margins (and fissures). Near the enamel�dentine junction, hypomineralized regions with a prismatic appearance are found as enamel tufts. This protein is wealthy in proline and glutamine, and is 178 amino acids in length with a hydrophobic core and protein� protein interaction area. Within the enamel matrix, it self-assembles into spherical nanospheres that lie between the hydroxyapatite crystals, performing as spacers that allow the crystals to develop as enamel matures. It has a hydrophilic, mineral-binding area, binding tightly to the enamel crystals by way of the C-terminal, which is cleaved shortly after secretion. This is the important thing to regulating crystal development, as these nanospheres promote growth of the hydroxyapatite crystals, preventing premature crystal�crystal fusion. Non-amelogenins the remaining proteins forming a small (10%) part of the natural matrix are grouped together as non-amelogenins. These embrace enamelin, tuftelin and ameloblastin: � Enamelin is the most important enamel protein and is an acidic glycoprotein. It is rapidly processed after secretion and should interact with enamel crystals and be involved with nucleation, though proof of that is limited. Ameloblastin cleavage products missing the C-terminus have been discovered to accumulate at the prism boundary throughout the enamel layer. Enamel matrix incorporates metalloproteinases throughout early enamel improvement and serine proteinases in the course of the late stages of enamel formation. It is secreted from the secretory face of the Tomes course of directly into the enamel matrix. Amelogenin Approximately 20% of younger, growing enamel is nearly all proteinaceous. The majority of the creating enamel organic matrix are amelogenins, secreted by the ameloblasts. In the maturation section, the matrix proteins have a lowered position to play, as most organic material has been degraded and misplaced. Such degraded matrix proteins could accumulate in the extracellular house across the ameloblast cells where they might inhibit cell activity and so management or restrict the thickness of enamel deposition. Nucleation Nucleation is the mechanism whereby a hydroxyapatite crystal is seeded onto the organic matrix, allowing it to develop at the expense of calcium and phosphate surrounding it. In enamel, the process of heterogeneous nucleation, also referred to as epitactic nucleation (epitaxis), occurs. This is outlined as the expansion of one crystalline substance on a unique strong floor having related lattice spacings, the organic matrix. Post-maturation stage Once maturation of the enamel is full, the ameloblasts bear additional adjustments in morphology associated with modifications in function, which could be considered as the post-maturation stage.
References - Skinner DB: En bloc resection for neoplasms of the esophagus and cardia. J Thorac Cardiovasc Surg 85:59, 1983.
- Kim TS, Chung JW, Park JH, et al: Renal artery evaluation: comparison of spiral CT angiography to intra-arterial DSA, J Vasc Interv Radiol 9(4):553-559, 1998.
- Kass DA, Maughan WL: From ìEmaxî to pressure-volume relations: A broader view, Circulation 77:1203, 1988.
- Jiang X, Anderson C, Schnatz PF: The safety of direct trocar versus Veress needle for laparoscopic entry: a meta-analysis of randomized clinical trials, J Laparoendosc Adv Surg Tech A 22(4):362-370, 2012.
- Yanagimachi R, Yanagimachi H, Rogers BJ: The use of zona-free animal ova as a test-system for the assessment of the fertilizing capacity of human spermatozoa, Biol Reprod 15:471n476, 1976.
- Manecke GR Jr, Kotzur A, Atkins G, et al: Massive pulmonary hemorrhage after pulmonary thromboendarterectomy, Anesth Analg 99:672, 2004.
- Sacco RL, Diener HC, Yusuf S, et al. Aspirin and extended-release dipyridamole versus clopidogrel for recurrent stroke. N Engl J Med 2008;359(12):1238-51.
- Burgess EM. Immediate postsurgical prosthetic fitting: a system of amputee management. Phys Ther 1971;51(2):139-143.
|