|
Dr Daniel Conway - Dept of Anaesthesia
- Manchester Royal Infirmary
- Manchester
Kemadrin dosages: 5 mg
Kemadrin packs: 20 pills, 30 pills, 60 pills, 90 pills, 180 pills, 270 pills, 360 pills

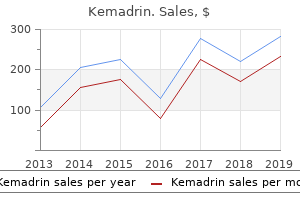
Kemadrin 5mg on-lineRitz E medications 319 order kemadrin 5mg overnight delivery, Rychlik I, Locatelli F, et al: End-stage renal failure in kind 2 diabetes: a medical catastrophe of worldwide dimensions. Schwenger V, Mussig C, Hergesell O, et al: Incidence and medical characteristics of renal insufficiency in diabetic sufferers. Nakano S, Ogihara M, Tamura C, et al: Reversed circadian blood pressure rhythm independently predicts end-stage renal failure in non-insulin-dependent diabetes mellitus topics. Rossing P, Hougaard P, Borch-Johnsen K, et al: Predictors of mortality in insulin dependent diabetes: 10-year follow-up study. Melin J, Hellberg O, Larsson E, et al: Protective impact of insulin on ischemic renal harm in diabetes mellitus. Chantrel F, Enache I, Bouiller M, et al: Abysmal prognosis of sufferers with type 2 diabetes getting into dialysis. Inomata S, Itoh M, Imai H, et al: Serum ranges of erythropoietin as a novel marker reflecting the severity of diabetic nephropathy. Tong Z, Yang Z, Patel S, et al: Promoter polymorphism of the erythropoietin gene in severe diabetic eye and kidney problems. Watanabe D, Suzuma K, Matsui S, et al: Erythropoietin as a retinal angiogenic factor in proliferative diabetic retinopathy. Koch M, Thomas B, Tsch�pe W, et al: Survival and predictors of dying in dialysed diabetic patients. Tozawa M, Iseki K, Iseki C, et al: Pulse pressure and risk of total mortality and cardiovascular events in sufferers on continual hemodialysis. Standl E, Schnell O: A new have a look at the heart in diabetes mellitus: from ailing to failing. Hosoda Y, Yamamoto T, Takazawa K, et al: Coronary artery bypass grafting in sufferers on persistent hemodialysis: surgical outcome in diabetic nephropathy versus nondiabetic nephropathy sufferers. Le Feuvre C, Dambrin G, Helft G, et al: Clinical consequence following coronary angioplasty in dialysis sufferers: a case-control examine within the era of coronary stenting. Hatada K, Sugiura T, Nakamura S, et al: Coronary artery diameter and left ventricular operate in sufferers on maintenance hemodialysis remedy: comparison between diabetic and nondiabetic patients. Ritz E, Koch M: Morbidity and mortality as a result of hypertension in sufferers with renal failure. Solders G, Tyd�n G, Tibell A, et al: Improvement in nerve conduction 8 years after combined pancreatic and renal transplantation. Morath C, Zeier M, Dohler B, et al: Metabolic control improves long-term renal allograft and affected person survival in type 1 diabetes. Christiansen E, Vestergaard H, Tibell A, et al: Impaired insulinstimulated nonoxidative glucose metabolism in pancreas-kidney transplant recipients. Foger B, Konigsrainer A, Palos G, et al: Effects of pancreas transplantation on distribution and composition of plasma lipoproteins. Midtvedt K, Hjelmesaeth J, Hartmann A, et al: Insulin resistance after renal transplantation: the impact of steroid dose reduction and withdrawal. Morioka T, Emoto M, Tabata T, et al: Glycemic control is a predictor of survival for diabetic sufferers on hemodialysis. Inaba M, Okuno S, Kumeda Y, et al: Glycated albumin is a greater glycemic indicator than glycated hemoglobin values in hemodialysis sufferers with diabetes: impact of anemia and erythropoietin injection. Koch M, Trapp R, Kulas W, et al: Critical limb ischaemia as a primary reason for death in sufferers with end-stage renal disease: a singlecentre examine. Schwenger V, Morath C, Salava A, et al: Damage to the peritoneal membrane by glucose degradation products is mediated by the receptor for superior glycation end-products. Rippe B, Simonsen O, Heimburger O, et al: Long-term medical results of a peritoneal dialysis fluid with much less glucose degradation products. Tyden G, Bolinder J, Solders G, et al: Improved survival in sufferers with insulin-dependent diabetes mellitus and end-stage diabetic nephropathy 10 years after mixed pancreas and kidney transplantation. Fedele D: Therapy insight: sexual and bladder dysfunction related to diabetes mellitus. Bonadio M, Costarelli S, Morelli G, et al: the affect of diabetes mellitus on the spectrum of uropathogens and the antimicrobial resistance in elderly adult sufferers with urinary tract an infection. Kofoed-Enevoldsen A, Borch-Johnsen K, Kreiner S, et al: Declining incidence of persistent proteinuria in kind 1 (insulindependent) diabetic patients in Denmark. Borch-Johnsen K, N�rgaard K, Hommel E, et al: Is diabetic nephropathy an inherited complication Carr S, Mbanya J-C, Thomas T, et al: Increase in glomerular filtration fee in sufferers with insulin-dependent diabetes and elevated 1321. Lurbe E, Redon J, Kesani A, et al: Increase in nocturnal blood stress and development to microalbuminuria in type 1 diabetes. Kosugi T, Nakayama T, Heinig M, et al: Effect of decreasing uric acid on renal illness in the sort 2 diabetic db/db mice. Although the stones appear to be localized to the urinary tract, urolithiasis is actually a systemic disease. While the surgical remedy of urolithiasis has tremendously advanced over time, the necessity to perceive how stones form continues to be of critical importance because they are often prevented from recurring. Overall, the metabolic evaluation of urolithiasis remains to be not carried out typically enough, in our opinion. In addition to the potential of uncovering treatable underlying diagnoses, the pathophysiologic definition of kidneys also can guide choice and assist monitor therapy. Age-adjusted prevalence was proven to be larger in southern elements of the United States. The contribution of mineral content and high quality of the water to the prevalence of kidney stones and its geographic distribution was questioned by a examine in three Midwest U. Prevalence information from 1988 to 1994 was not capable of use dietary elements to explain geographic variation within the prevalence of kidney stone diseases. According to the latest estimate, 1 in 11 individuals in the United States had a historical past of kidney stones, in distinction to a earlier estimate of 1 in 20 U. Aside from gender, race, age, ethnicity, and socioeconomic class, conditions associated with metabolic syndrome have been proven to be predictive of kidney stone illness. Furthermore, weight problems, diabetes, gout, and low household earnings ($19,999) have been extra likely to be associated with kidney stone illness. The affiliation between features of the metabolic syndrome, including obesity and diabetes, and the prevalence of kidney stone illness is according to a previous prospective examine, which indicated that the risk of kidney stone illness increased with weight problems and weight gain. Brikowski and associates12 took a different (and attention-grabbing approach) using international warming trends; they modeled the northward growth of the U. A retrospective evaluation of 1201 stone formers up to now 3 decades has proven that over time, elevated incidence of calcium phosphate stones coincides with increased urinary pH and the number of shock wave lithotripsy therapies. The position of dietary calcium as a threat factor was assessed in a few prospective observational research displaying that low dietary calcium consumption is related to a better threat of kidney stones in girls in addition to young men. In adult populations, one small examine from Minnesota confirmed an incidence rate of a hundred and one. It has also been reported that youngsters are presently consuming less water than up to now. However, a high prevalence of obesity, diabetes, and hypertension is commonly associated with uric acid urolithiasis in Western societies29-31 and has additionally been shown to be present in Hmong populations born in the United States.
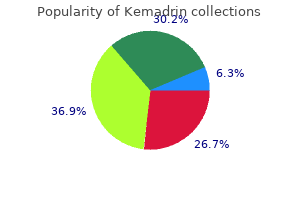
Order 5 mg kemadrin with amexAt the top of every section medicine hat lodge purchase kemadrin 5mg with mastercard, Consults are presented succinctly to illustrate how this approach is used on the bedside. Hence data must be interpreted in the context of the prevailing stimulus and the "anticipated" renal response. This is an arbitrary definition based on comparing the 24-hour urine quantity with traditional values noticed in individuals who eat a typical Western food regimen. The magnitude of this force is big, in that a difference of 1 mOsm/kg H2O generates a pressure of about 19. Because the interstitial osmolality rises threefold (from 300 to 900 mOsmol/kg H2O) within the outer medulla, two thirds, or three L of the 4. As calculated beforehand, 27 L/day are delivered to the distal nephron in a standard subject, and the urine flow fee throughout maximum water diuresis is round 10 to 15 mL/min (14 to 22 L/day). If the urine volume is significantly lower than 10 L/day, one should look for a reason for decreased distal supply of filtrate. The purpose is that the medullary interstitial osmolality is prone to be decrease owing to a prior medullary washout during the water diuresis. In subjects eating a typical Western food plan, the speed of excretion of osmoles is 600 to 900 mOsm/day, with electrolytes and urea each accounting for close to half of the urine osmoles. Therefore during a water diuresis, a change within the Uosm may replicate a change in the osmole excretion fee and/or in the volume of filtrate delivered to the distal nephron (which largely determines the urine quantity on this setting). For example, if the speed of excretion of osmoles is 800 mOsm/day, the Uosm is 50 mOsm/L if the 24-hour urine volume is sixteen L, and 100 mOsm/L if the 24-hour urine volume is eight L. Note that although the balances for Na+ + K+ and for water are very different in these three examples, calculation of electrolyte-free water reveals a negative steadiness of 2 L of electrolyte-free water in all of them. The goals for therapy-to correct the hypernatremia and to return the quantity and the composition of the extracellular and intracellular fluid compartments to their regular values-are clear solely after a tonicity stability is calculated. Calculation of the electrolyte-free water stability relies on how a lot water is needed to make all the Na+ + K+ into an answer with a tonicity equal to the normal plasma tonicity. To perform this calculation, one must know the volume of and the concentrations of Na+ + K+ within the enter and within the urine. With regard to the output, this patient excreted 1 L of isotonic salt solution and a pair of L of electrolyte-free water. In sensible terms, a tonicity stability can be performed solely in a hospital setting, where inputs and outputs are precisely recorded. Nevertheless, proscribing the evaluation of the output to the urine data can be adequate in an acute setting. Therefore, the objective of therapy is to induce a negative steadiness of 300mmol of Na+ while sustaining water balance. Circulating vasopressinase Non-osmotic stimuli -Low efficient arterial blood quantity -Pain, anxiousness, medicine. Since his head injury, his urine output had been persistently about four L/day and his Uosm round 200 mOsm/kg H2O in a number of 24-hour urine collections. He noted that if he stopped ingesting water after supper, his sleep was not interrupted by a must void. An important part of this workup is to decide in a affected person with hypernatremia whether thirst is current; its absence suggests that the defect entails the hypothalamic osmostat (tonicity stat is a better term as a outcome of it refers only to effective osmoles; i. Step four: Establish the Basis for Nephrogenic Diabetes Insipidus � Is this a water diuresis A 16-year-old male (weight 50 kg, complete body water 30 L) underwent craniopharyngioma resection within the morning. Such a lesion may clarify why polyuria was not current in a single day if the affected person stopped water consumption a quantity of hours prior to going to sleep. Its basis probably was a "discovered behavior" to avoid the uncomfortable feeling of thirst. Calculate the tonicity stability: Water Balance: the patient acquired three L of isotonic saline, and therefore had an input of 3 L of water. Na+ + K+ Balance: the affected person received 450 mmol (3 L � a hundred and fifty mmol Na+/L) and excreted solely one hundred fifty mmol (3 L urine � 50 mmol Na+/L). Urea may be also an effective urine osmole if the speed of excretion of electrolytes is low. The "anticipated" medullary interstitial osmolality is about 600 mOsm/kg H2O at considerably high osmole excretion rates, and values nearer to the Posm are observed at a lot higher osmole excretion charges. Osmole Excretion Rate In an adult during an osmotic diuresis, the speed of excretion of osmoles ought to be much higher than a thousand mOsm/day (more than zero. Not all osmoles, nevertheless, are equal of their ability to increase the urine volume. The internet results of excreting some further urea is the next Uosm but not a better urine move fee. Urine move price = # effective urine osmoles efficient Uosm (2) the character of the urine osmoles should be determined by measuring the speed of excretion of the individual osmoles in the urine. One can deduce which solute is likely to be responsible for the osmotic diuresis by measuring their concentrations in plasma. A salineinduced osmotic diuresis might happen if there was a big infusion of saline or in a affected person who has cerebral or renal salt wasting. Sources of the Urine Osmoles In a affected person with a glucose- or a urea-induced osmotic diuresis, it is important to resolve whether these osmoles have been derived from an exogenous supply or from catabolism of endogenous proteins. The former may be calculated from the rise within the focus of urea in plasma (Purea) and assuming a quantity of distribution of urea equal to total body water (60% of body weight within the absence of obesity). One can use the following calculation to determine whether or not the supply of urea was the breakdown of exogenous or endogenous proteins, if the intake of proteins is thought. Because every mmol of urea incorporates two atoms of nitrogen, about 570 mmol of urea could be produced from the oxidation of 100 g of protein. In terms of lean physique mass: Water is the main constituent within the physique (80% of weight): every kg has 800 g of water and a hundred and eighty g of protein. Hence, to produce enough glucose from protein to induce 1 L of osmotic diuresis (300 mmol of glucose), one would want the catabolism of 90 g of protein (equivalent to the catabolism of 1 lb of lean physique mass). One also wants to determine whether sufficient mannitol was administered to trigger the observed diploma of polyuria. Step 3: Identify the Source of the Osmoles within the Urine In a patient with a glucose- or urea-induced osmotic diuresis, it is necessary to resolve whether these osmoles were derived from an endogenous source or from catabolism of exogenous proteins. The clinician ought to concentrate on hidden glucose within the lumen of the gastrointestinal tract, as a end result of it could soon be absorbed and contribute to the osmotic diuresis. In a affected person with a saline-induced osmotic diuresis, one should determine why a lot NaCl is being excreted. Some potential causes are prior extreme saline administration (a common scenario in a hospital setting), administration of a loop diuretic in a patient with important edema, cerebral salt losing, and renal salt wasting. In the past 48 hours, she was thirsty, drank large volumes of fruit juice, and noted that her urine quantity was very excessive. The caveat right here, however, is that the Uosm from a spot urine sample will not be consultant of the value of the Uosm throughout the 24-hour period if there are intermittent intervals of water diuresis.
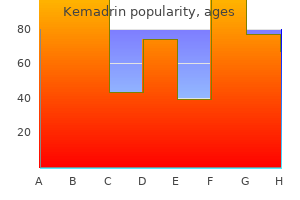
Buy genuine kemadrinSimilarly kapous treatment buy on line kemadrin, adrenalectomized canine receiving replacement of mineralocorticoids still have abnormal water excretion. A direct impact of glucocorticoid deficiency that enhances water permeability of the amassing duct has been proposed, but such a concept has not been supported by studies of anuran membranes suggesting that glucocorticoids enhance quite than inhibit water transport. The frequency of hyponatremia on this population of sufferers is unknown, but in a survey conducted in a single giant psychiatric hospital, 20 polydipsic sufferers with a serum [Na+] lower than 124 mEq/L have been reported,350 and another survey discovered hyponatremia in 8 of 239 patients. The relative contributions of the pharmacologic agent and the psychosis are subsequently difficult to define, as a outcome of thiazides and carbamazepine are additionally frequently implicated. Although this has been ascribed to a rise in fluid intake within the setting of very low solute intake,357 such sufferers may have sustained important solute losses. A multivariate evaluation revealed that weight acquire associated to extreme fluid consumption was the strongest single predictor of the hyponatremia. Chlorpropamide between antipsychotic medicine and hyponatremia is regularly encountered, the pharmacologic agents themselves may not be the principal components answerable for the water retention. Antineoplastic Drugs the incidence of delicate hyponatremia in patients taking chlorpropamide may be as high as 7%, but severe hyponatremia (<130 mEq/L) happens in 2% of patients so treated. The incidence of hyponatremia in carbamazepine-treated sufferers was believed to be as excessive as 21%, however a survey of sufferers with mental retardation reported a lower incidence of 5%. In this latter research, involving seventy five sufferers, 12% developed hyponatremia (serum [Na+] < one hundred thirty five mmol/L). Therefore, though a medical affiliation Since the Nineteen Forties, it has been known that the administration of opioid agonists, corresponding to morphine, reduces urine move by causing the discharge of an antidiuretic substance. The possibility that endogenous opioids might function potential neurotransmitters has been instructed by the discovering of enkephalins in nerve fibers projecting from the hypothalamus to the pars nervosa. The causes for these various observations may be that the opiates and their receptors are broadly distributed within the mind, implying that the location of action of the opiate can differ markedly, depending on the route of administration. In one study, sixteen of 17 sufferers had ranges under 4 mg/dL, whereas in 13 sufferers with hyponatremia of other causes the extent was higher than 5 mg/dL. Concomitant with the water retention, an increment in urinary Na+ excretion was noted. The relative contributions of the water retention and Na+ loss to the event of hyponatremia have been subsequently investigated. Acute water loading causes transient natriuresis however, when water intake is increased more slowly, no vital negative Na+ loss could be documented. These studies have clearly demonstrated that the hyponatremia is mainly a consequence of water retention; however, it have to be noted that the online improve in water steadiness fails to account entirely for the decrement in serum [Na+]. The integrity of renal regulation of Na+ stability is manifested by the power to conserve Na+ throughout Na+ restriction and by the traditional excretion of a Na+ load. Since the original report of Schwartz and coworkers,405 the syndrome has been described in an rising variety of clinical settings (Table sixteen. In addition, an rising variety of sufferers with acquired immunodeficiency syndrome have been reported to have hyponatremia. Regression analyses have proven that the precision and sensitivity of this response are primarily the identical as these in healthy topics, except that the intercept or threshold value at 253 mOsm/kg is well below the normal range. This pattern, which reflects the resetting of the osmoreceptor, was present in 9 of 25 sufferers who had a analysis of bronchogenic carcinoma, cerebrovascular illness, tuberculous meningitis, acute respiratory disease, or carcinoma of the pharynx. Another affected person was reported with hyponatremia and acute idiopathic polyneuritis who reacted in an similar method to the hypertonic saline infusion and was decided to have resetting of the osmoreceptor. Because their threshold operate is retained once they obtain a water load, this affected person and others with reset osmostats have been in a position to dilute their urine maximally and maintain a urine circulate sufficient to forestall an additional improve in physique water. Although gastrointestinal complaints typically happen early, many of the manifestations of hyponatremia are neurologic, together with lethargy, confusion, disorientation, obtundation, and seizures, designated as hyponatremic encephalopathy. The cerebral edema can also trigger a neurogenic pulmonary edema and hypoxemia,440 which might in turn increase the severity of mind swelling. Older persons and young kids with hyponatremia are most likely to develop symptoms. It has also turn out to be apparent that neurologic issues happen more incessantly in menstruating ladies. In a case-control examine, Ayus and colleagues noted that despite an approximately equal incidence of postoperative hyponatremia in males and females, 97% of these with permanent brain harm had been women, and 75% of them had been menstruating. In this subgroup of symptomatic sufferers, the mortality was no different from that of asymptomatic sufferers (9% to 10%). In the hyponatremic patients, demise incessantly occurred after the plasma [Na+] was returned to normal and was generally thought to be due to the progression of extreme underlying illness; this means that the hyponatremia is an indicator of severe illness and poor prognosis. Equally controversial is the mortality price related to hyponatremia in kids. One series discovered no in-hospital deaths attributable to hyponatremia, however others described an 8. In reality, such cerebral edema occasionally causes herniation, as has been famous in postmortem examination of each people and experimental animals. This process is prone to account for the extra marked cerebral dehydration that accompanies the correction in previously tailored animals. This could also be as a end result of the extra rapid reac- cumulation of organic osmolytes, and notably myoinositol in the azotemic state. The purpose for the profound differences between the symptoms of acute and persistent hyponatremia is now nicely understood to be brought on by the method of mind quantity regulation described above. One report discovered a reasonably high incidence of symptoms in 223 sufferers with continual hyponatremia as a end result of thiazide administration-49% had malaise-lethargy, 47% had dizzy spells, 35% had vomiting, 17% had confusion-obtundation, 17% experienced falls, 6% had headaches, and 0. Because thiazide-induced hyponatremia may be readily corrected by stopping the thiazide and/or administering sodium, this represents a super scenario by which to assess enchancment in hyponatremia symptomatology with normalization of the serum [Na+]; on this examine, all these signs improved with correction of the hyponatremia. Even in sufferers adjudged to be "asymptomatic" by virtue of a normal neurologic examination, accumulating proof means that there could additionally be beforehand unrecognized adverse effects because of chronic hyponatremia. The clinical significance of the gait instability and fall data have been indicated by a number of impartial research that demonstrated elevated rates of bone fractures in sufferers with hyponatremia. Various formulas have been suggested for calculating the initial price of infusion of hypertonic solutions,460 however there has been no consensus regarding optimal infusion charges of 3% NaCl. This was recommended by a consensus conference organized to develop guidelines for prevention and treatment of exerciseinduced hyponatremia, an acute and probably deadly situation,465 and adopted as a common recommendation by an expert panel. In a retrospective review of patients who introduced with extreme neurologic signs and serum [Na+] lower than a hundred twenty five mmol/L, immediate therapy with isotonic or hypertonic saline resulted in a correction of about 20 mEq/L over several days and neurologic restoration in almost all cases; in distinction, in sufferers who have been handled with fluid restriction alone, there was very little correction over the examine period (<5 mEq/L over 72 hours), and the neurologic outcomes had been a lot worse, with most of those sufferers dying or coming into a persistent vegetative state. Brain herniation, essentially the most dreaded complication of hyponatremia, is seen almost completely in patients with acute hyponatremia (usually <24 hours) or in sufferers with intracranial pathology. Because of this adaptation course of, persistent hyponatremia is arguably a situation that clinicians assume they may not have to be as involved about, which has been bolstered by widespread usage of the descriptor asymptomatic hyponatremia for so much of of these patients. An further purpose to treat even asymptomatic hyponatremia effectively is to prevent a lowering of the serum [Na+] to more symptomatic and dangerous ranges throughout treatment of underlying conditions. Predictors of Likely Failure of Fluid Restriction � Highurineosmolality(>500mOsm/kgH2O).
5 mg kemadrin overnight deliveryThe main end result symptoms 0f ms kemadrin 5 mg overnight delivery, a composite of dying from cardiovascular causes or hospitalization for heart failure had occurred in 914 patients (21. Vaptans are small, orally active, nonpeptide molecules that lack agonist effects and show excessive affinity for and specificity to their corresponding receptors. In one research, patients treated with tolvaptan, and who had an increase in serum Na+ of two mmol/L or more, had half the mortality price of those with no improvement in serum Na+ stage 2 months after discharge. However, the trial was terminated early owing to an extreme mortality fee in the remedy group. To date, this concept has been evaluated in one potential observational and one multicenter, randomized, double-blind, placebo-controlled study. These include the potential for long-term efficacy, use in volume overload in the setting of preserved ejection fraction with a nondilated ventricle, position in possible loop diuretic dose sparing, period of therapy, and dosing over the quick and long term. Three teams of vasoconstrictors have been studied-vasopressin V1 receptor analogues. On the basis of the pathophysiologic options of renal vasoconstriction in opposition to a background of systemic and, particularly, splanchnic arterial vasodilation, specific remedies consist broadly of renal vasodilators and systemic vasoconstrictors. The these agents cause marked vasoconstriction by way of their action on the V1 receptors current within the smooth muscle of the arterial wall. They are used extensively for the management of acute variceal bleeding in patients with cirrhosis and portal hypertension. In nonresponders, who are inclined to have more severe cirrhosis (Child-Pugh rating > 13), size of survival is notably reduced. However, long-term management of these managements with vasoconstrictors is impractical. In virtually all research, terlipressin was given till serum creatinine levels decreased to less than 1. So far, only one case sequence has been reported, by which three patients had been maintained on terlipressin for 2 months till liver transplantation. A key target for predicting prognosis appears to be the response in mean arterial stress at three days after mixed terlipressin-albumin remedy. In a small study, sufferers whose imply arterial strain rose 10 mm Hg or extra from baseline had much less requirement for dialysis and larger incidence of liver transplantation than these with smaller responses in imply arterial stress. More importantly, this response was related to better short-term and long-term general survival and transplant-free survival. All patients acquired vasoactive agents, as acceptable, and have been followed for as a lot as 5 days postoperatively. Compared to the management group, terlipressin infusion was related throughout the examine period with important will increase in imply arterial stress, systemic vascular resistance and renal operate, considerably decreased coronary heart rate, cardiac output, hepatic and renal arterial resistive indices, portal venous blood flow, and use of vasoconstrictor medication throughout reperfusion. Unfortunately, regardless of the favorable results of terlipressin, a serious downside is its unavailability in many countries, including the United States and Canada. Only one small randomized, controlled trial553 involving a direct comparability has been reported in abstract type. In this research, terlipressin plus albumin was significantly simpler than octreotide, midodrine, and albumin, both by method of improved renal operate (75% vs. Responses to each agents had been related in phrases of imply arterial stress and renal function. In one meta-analysis, any vasoconstrictor with albumin was superior to albumin alone or no lively therapy, both for improvement in renal operate and reduced all-cause mortality. However, the result measures assessed have been goal, which lowered the risk of bias. To date, a quantity of studies performed in animals and sufferers with cirrhosis have yielded promising results. Of patients who acquired the 200-mg dose, 50% achieved a normal serum Na+ level (136 mmol/L). In the opposite trial, 33 cirrhotic sufferers received lixivaptan in doses of fifty to 500 mg, with a dose-response effect; nevertheless, even at the highest dose, the overall response was modest (serum Na+ level elevated from a hundred twenty five � 1 to 132 � 1 mmol/L). Three randomized controlled trials exploring the effects of satavaptan, alone or in combination with diuretics, in a total of 1200 cirrhotics with uncomplicated or difficult to treat ascites have been carried out. The specific position of satavaptan in the increased mortality was uncertain, given that almost all deaths had been because of problems of cirrhosis. Overall, the effects of vaptans in cirrhotics seem to be modest; this phenomenon could also be explained by avid proximal tubular solute reabsorption leading to decreased distal delivery or by V2 receptor�independent pathways of water retention. The risk of mixture or sequential therapies has also been examined in preliminary studies. Whether mixture remedy can preclude the need for liver transplantation or significantly improve survival remains to be investigated. The benefits, if any, by method of prolonging survival, are doubtful,742 and the incidence of morbidity ensuing from these therapies is excessive. The hemodynamic effects have been thought to be mediated by clearance of vasoactive substances. Predictors of renal recovery included younger recipient and donor, nonalcoholic liver illness, and low posttransplantation bilirubin degree. In this regard, the query of mixed liver-kidney transplantation turns into important. Data from the United Network for Organ Sharing have shown higher rates of 5-year survival after liver-kidney transplantation than after liver transplantation alone in patients with pretransplantation serum creatinine ranges higher than 2. In distinction, single-center outcomes were related, regardless of pretransplantation renal function. Therefore, the standards for donor allocation have to be modified to incorporate these elements into the final rating for prioritization. Rakova N, Juttner K, Dahlmann A, et al: Long-term space flight simulation reveals infradian rhythmicity in human Na(+) stability. Parati G, Esler M: the human sympathetic nervous system: its relevance in hypertension and coronary heart failure. Arroyo V, Fernandez J: Management of hepatorenal syndrome in sufferers with cirrhosis. Rami K: Aggressive salt and water restriction in acutely decompensated heart failure: is it price its weight in salt Sola E, Cardenas A, Gines P: Results of pretransplant therapy of hepatorenal syndrome with terlipressin. Ziomber A, Machnik A, Dahlmann A, et al: Sodium-, potassium-, chloride-, and bicarbonate-related results on blood pressure and electrolyte homeostasis in deoxycorticosterone acetate-treated rats. Machnik A, Neuhofer W, Jantsch J, et al: Macrophages regulate salt-dependent volume and blood strain by a vascular endothelial development factor-C-dependent buffering mechanism. Schafflhuber M, Volpi N, Dahlmann A, et al: Mobilization of osmotically inactive Na+ by development and by dietary salt restriction in rats. Titze J: Water-free Na+ retention: interaction with hypertension and tissue hydration.
Diseases - Leukocyte adhesion deficiency syndrome
- Urethral obstruction sequence
- Leigh disease
- Duodenal atresia
- Palmoplantar porokeratosis of Mantoux
- Idiopathic alveolar hypoventilation syndrome
- Peripheral nervous disorder
- Scholte Begeer Van Essen syndrome
Order kemadrin cheap onlineA history of coronary artery interventions medications errors generic 5mg kemadrin free shipping, significant arrhythmias, or insertion of a pacemaker or defibrillator ought to be recognized. It is imperative that any history of resting or exertional chest ache and/or shortness of breath be recognized. A historical past of claudication, peripheral ulcers, revascularization, gangrenous extremities, or extremity amputation should be documented. The interpretation of weight change is sophisticated, nevertheless, because lack of physique mass may be masked by fluid accumulation. Medications ought to be reviewed for potential nephrotoxic results and for applicable dosing for renal perform. When diabetes exists, its duration, particular medications, adequacy of management, hemoglobin A1C ranges, and results of microalbuminuria research ought to be ascertained. In basic, the onset of kind 2 diabetes is tough to determine as a end result of this disease may be clinically silent for years. A historical past of high or low blood pressure extremes, as nicely as response to and adherence to antihypertensive medication regimens, must be documented. Fever, skin rash, inflammation of the eyes or sinuses, and joint pains increase the possibility of secondary forms of glomerulonephritis. The multiple extrarenal manifestations of polycystic kidney illness embrace cerebral aneurysms, which are the most lifethreatening extrarenal complication. Because these aneurysms occur extra commonly within families, a history of cerebral aneurysms, stroke, or sudden dying at a young age amongst relations ought to be sought. Colonic diverticula and stomach wall or inguinal hernias are additionally frequent in these sufferers. Although overt hypotension is the strongest indicator of attainable renal underperfusion, an orthostatic pulse enhance of greater than 30 beats/min (measured 1 minute after standing) is indicative of less extreme quantity depletion. Dry axillae and dry mucous membranes with a furrowed tongue are useful indicators of quantity depletion. At the opposite excessive, hypertension, peripheral edema, pleural effusions, and pulmonary rales could indicate volume overload and require remedy with diuretics or ultrafiltration. Heart failure and cirrhosis also generate whole physique salt and water growth, with efficient intraarterial quantity contraction. The cardiac examination could reveal left ventricular hypertrophy or decompensation. Costovertebral tenderness indicates attainable inflammatory or infectious kidney illness. Skin necrosis brought on by calcific arteriopathy and calciphylaxis is a dreaded complication. Excretion of greater than 3000 mg/day of protein (primarily albumin) is most consistent with a glomerular course of. Quantitative measurement of protein and creatinine excretion could additionally be very helpful in chosen patients. Evaluation of complement ranges may be helpful with certain forms of glomerulonephritis. In general, a timed urine assortment to measure creatinine clearance is the standard methodology for documenting renal glomerular perform. A timed urine assortment for urea nitrogen can be obtained to judge dietary status by estimating a protein catabolic rate. Although it could have some advantage relative to creatinine focus, this stays unproven. Hematuria with high-grade proteinuria suggests a glomerular process, whereas low-grade proteinuria is according to nephrosclerosis, an interstitial illness, or polycystic disease. With the idea that urine creatinine excretion is about 1 g/day, this ratio, expressed as grams of protein per gram of creatinine, represents the daily protein excretion in grams per day. The sonogram supplies a kidney measurement evaluation, provides data on cortical width and echogenicity, and demonstrates the presence or absence of scars and hydronephrosis, in addition to renal stones or plenty. Other voiding symptoms similar to difficulty voiding, polyuria, halting voiding signs, or frequent small voids additionally happen. The patient might complain of grossly purulent, foul-smelling, and/or blood-tinged or frankly bloody urine. Some sufferers can describe prior infecting organisms as demonstrated on urine culture. In addition to localizing symptoms of ache, with or with out fever, some patients have constitutional signs of fatigue, malaise, and weight reduction. Gastrointestinal symptoms of nausea and vomiting, constipation, or diarrhea may be current. High-risk groups embrace pregnant girls, sexually lively younger girls, older adults, notably in a nursing home setting, patients with indwelling urinary catheters or different drainage gadgets, sufferers with diabetes, and sufferers with spinal twine injury. Current suggestions are that solely pregnant ladies should be screened (and treated) for asymptomatic bacteriuria. These embody pregnancy, diabetes, renal transplantation, and long-term immunosuppression. The affected person with a severe systemic infection of urinary origin might have a poisonous look and altered mentation. Careful consideration ought to be given to the back, flank, abdomen, and pelvic areas to detect localized tenderness or a palpable mass. On the urine dipstick take a look at, the pH can be markedly alkaline (supraphysiologic degree; i. Urine granulocytes typically point out inflammation, which can or will not be as a outcome of an infection. They could be detected by a dipstick take a look at for leukocyte esterase, an enzyme contained in the granules of neutrophils. In rare cases, false-positive results are produced by strong oxidants in the urine collection container. High-grade proteinuria or glucosuria, some antibiotics, and excessive levels of ascorbic acid can produce false-negative results. A finding of marked proteinuria raises the potential of reflux nephropathy sophisticated by focal glomerulosclerosis, whereas average proteinuria (in the range of one thousand to 1500 mg/day or less) can occur with chronic interstitial nephritis. The spun urine sediment reveals neutrophils, usually in clumps, and sometimes neutrophil casts. A Gram-stained smear of unspun urine or spun sediment can aid in identification of the micro organism and assist goal empirical therapy. Good urine collection and culture techniques are essential to keep away from contamination. Midstream urine should be collected after cautious washing of exterior genitalia followed by voiding right into a sterile container.
Buy generic kemadrin pillsThe diagnosis of orthostatic proteinuria requires that protein excretion throughout recumbency be less than 50 mg throughout those 8 hours symptoms bladder cancer order kemadrin in india. Few convincing data exist on the usefulness of comparing urinary protein to creatinine ratio measurements throughout recumbency versus ambulation as a diagnostic test for orthostatic proteinuria. Twenty-year follow-up of orthostatic proteinuria suggests a benign long-term course. It is present in 50% of patients after 10 years and solely 17% of sufferers after 20 years. The proteinuria disappears in some patients, whereas others may have a extra ominous glomerular lesion that portends an antagonistic long-term outcome. These sufferers have to be evaluated periodically for as long as proteinuria persists. Hematuria can result from injury to the kidney or to one other site in the urinary tract. An acceptable definition of hematuria is more than two red cells per high-power area in centrifuged urine. The urine dipstick take a look at detects one or two red cells per highpower field and is a really delicate test. In patients with isolated asymptomatic hematuria without proteinuria or renal insufficiency, the hematuria resolves in 20% of instances; however, a few of these sufferers will develop hypertension and proteinuria. Glomerular hematuria, in distinction to hematuria brought on by damage elsewhere in the urinary tract, is characterised by misshapen purple cells that have been distorted by osmotic and chemical stress as purple blood cells cross by way of the nephron. The differential pathologic analysis of glomerular hematuria with out proteinuria, renal insufficiency, or red blood cell casts contains IgA nephropathy, skinny basement membrane nephropathy, hereditary nephritis, and histologically normal glomeruli. The remaining sufferers had mesangioproliferative glomerulonephritis, interstitial nephritis, or focal glomerulosclerosis. In distinction, 216 Chinese adults with isolated hematuria who underwent a kidney biopsy were much extra likely to have IgA nephropathy than any other lesion. The information showed that sufferers with a relatively regular serum creatinine level, hematuria, and proteinuria of less than 1 g protein per day had been most likely to have skinny basement membrane nephropathy, IgA nephropathy, or no identifiable renal lesion. When hematuria is accompanied by 1 to three g protein per day of proteinuria but no significant renal insufficiency, IgA nephropathy was the most likely cause. Patients with hematuria and a serum creatinine of greater than three mg/dL most frequently had aggressive glomerulonephritis with crescents. Specimens from sufferers with systemic lupus erythematosus were excluded from the analysis. Proliferative or necrotizing glomerulonephritis other than immunoglobulin A nephropathy or lupus nephritis. Includes causes of nephrotic syndrome such as membranous nephropathy and focal segmental glomerulosclerosis. Certain rules typically apply to the clinical prediction of the more than likely trigger. Gross hematuria is most commonly found in IgA nephropathy or hereditary nephritis. The potential advantages of kidney biopsy in patients with isolated hematuria embrace discount of patient and doctor uncertainty by confirming a particular prognosis. However, the extent of effacement seems to correlate extra with the duration of energetic nephrotic syndrome than with the magnitude of proteinuria. Nephrotic syndrome not only may be attributable to major (idiopathic) glomerular diseases but additionally may be secondary to numerous identifiable illness states (Table 32. Despite the variations in these causes, the lack of substantial quantities of protein in the urine leads to a shared set of abnormalities that comprise nephrotic syndrome (Tables 32. Medications and other chemicals Organic, inorganic, elemental mercury* Organic gold Penicillamine, bucillamine Street heroin Probenecid Captopril Nonsteroidal antiinflammatory medication Lithium Interferon- Chlorpropamide Rifampin Pamidronate Paramethadione (Paradione), trimethadione (Tridione) Mephenytoin (Mesantoin) Tolbutamide Phenindione Warfarin Clonidine Perchlorate Bismuth Trichloroethylene Silver Insect repellent Contrast media Anabolic steroids 2. Allergens, venoms, immunizing agents Bee sting Pollens Poison ivy and poison oak Antitoxins (serum sickness) Snake venom Diphtheria, pertussis, tetanus toxoid Vaccines 3. Infections Bacterial: poststreptococcal glomerulonephritis, infective endocarditis, shunt nephritis, leprosy, syphilis (congenital and secondary), Mycoplasma an infection, tuberculosis, chronic bacterial pyelonephritis with vesicoureteral reflux Viral: hepatitis B, hepatitis C, cytomegalovirus infection, infectious mononucleosis (Epstein-Barr virus infection), herpes zoster, vaccinia, infection with human immunodeficiency virus-1 Protozoal: malaria (especially quartan malaria), toxoplasmosis Helminthic: schistosomiasis, trypanosomiasis, filariasis four. This laboratory evaluates kidney biopsies from a base population of approximately 10 million all through the southeastern United States and centered in North Carolina. The expected white/black ratio in this renal biopsy population is approximately 2: 1. The most consistent tubular lesion is elevated protein and lipid resorption droplets in tubular epithelial cells. Conspicuous resorbed lipid in epithelial cells prompted the designation lipoid nephrosis for this illness prior to the popularity of the ultrastructural glomerular lesion. Electron Microscopy Glomeruli normally present no staining with antisera specific for IgG, IgA, IgM, C3, C4, or C1q. The most frequent optimistic discovering is low-level mesangial staining for IgM, sometimes accompanied by low-level staining for C3. During active nephrosis, the effacement often could be very in depth, with just a few scattered intact foot processes. The latter has effacement of podocyte foot processes (arrow) and microvillous projections of podocyte cytoplasm. When this issue was injected into rodents, proteinuria occurred with partial fusion of glomerular epithelial cell foot processes. In a gaggle of 89 adults older than age 60, hypertension, typically severe, in addition to renal insufficiency, were extra frequent. This same process has also been described with different compounds, including interferon,82 penicillins, and rifampin. In most of these patients, discontinuation of the offending drug leads to resolution of the proteinuria, but it could take weeks to months for full amelioration of pyuria and renal insufficiency. This is a crucial affiliation as a outcome of in some sufferers, removing of the allergen has resulted within the decision of the proteinuria. Of 42 sufferers with idiopathic nephrotic syndrome, sixteen had optimistic results on pores and skin checks for meals allergy. Of the 18 patients with renal failure for whom follow-up information were out there, all showed recovery of kidney operate, but solely after prolonged intervals of dialytic renal replacement therapy. Explanations for this phenomenon embrace marked lower in glomerular permeability because of extensive foot course of effacement, tubular obstruction from proteinaceous casts, and intrarenal hemodynamic adjustments. The rapidity of the development of proteinuria in some patients is associated with evidence of volume contraction with increased hematocrit and hemoglobin level. The erythrocyte sedimentation price is increased as a consequence of the hyperfibrinogenemia in addition to hypoalbuminemia. In youngsters, this form of remedy results in a whole remission with disappearance of proteinuria in over 90% of sufferers within four to 6 weeks of therapy. If the dose is changed to alternate-day dosing when remission has occurred, the dosage may be decreased in children from 60 mg/m2/day to 40 mg/m2/day. Of the 58 handled sufferers who showed a response, 24% never skilled relapse, 56% experienced relapse on a single occasion or occasionally, and only 21% had frequent relapses.
Buy kemadrin onlineCammalleri L symptoms 3 months pregnant order 5 mg kemadrin with amex, Malaguarnera M: Rasburicase represents a brand new software for hyperuricemia in tumor lysis syndrome and in gout. Giroux L, Bettez P, Giroux L: Mitomycin-C nephrotoxicity: a clinico-pathologic research of 17 instances. Jolivet J, Giroux L, Laurin S, et al: Microangiopathic hemolytic anemia, renal failure, and noncardiogenic pulmonary edema: a chemotherapy-induced syndrome. Madore F: Does plasmapheresis have a role in the administration of myeloma forged nephropathy Kamijo A, Sugaya T, Hikawa A, et al: Urinary excretion of fatty acid�binding protein reflects stress overload on the proximal tubules. Portilla D, Dent C, Sugaya T, et al: Liver fatty acid�binding protein as a biomarker of acute kidney injury after cardiac surgical procedure. Negishi K, Noiri E, Doi K, et al: Monitoring of urinary L-type fatty acid-binding protein predicts histological severity of acute kidney harm. Susantitaphong P, Siribamrungwong M, Doi K, et al: Performance of urinary liver-type fatty acid�binding protein in acute kidney damage: a meta-analysis. Pozzi Mucelli R, Bertolotto M, Quaia E: Imaging methods in acute renal failure. Nissim I, Horyn O, Daikhin Y, et al: Ifosfamide-induced nephrotoxicity: mechanism and prevention. Rossi R: Nephrotoxicity of ifosfamide-moving in the path of understanding the molecular mechanisms. Bilbao I, Charco R, Balsells J, et al: Risk elements for acute renal failure requiring dialysis after liver transplantation. Dalpiaz G, Nassetti C, Stasi G: Diffuse alveolar haemorrhage from a rare main renal-pulmonary syndrome: micropolyangiitis: case report and differential diagnosis. Arroyo V, Guevara M, Gines P: Hepatorenal syndrome in cirrhosis: pathogenesis and treatment. Cardenas A: Hepatorenal syndrome: a dreaded complication of end-stage liver illness. Alessandria C, Ottobrelli A, Debernardi-Venon W, et al: Noradrenalin vs terlipressin in sufferers with hepatorenal syndrome: a prospective, randomized, unblinded, pilot study. Tungsanga K, Boonwichit D, Lekhakula A, et al: Urine uric acid and urine creatine ratio in acute renal failure. Sanchez M, Bosch X, Martinez C, et al: Idiopathic pulmonaryrenal syndrome with antiproteinase 3 antibodies. Fiaccadori E, Lombardi M, Leonardi S, et al: Prevalence and scientific consequence associated with preexisting malnutrition in acute renal failure: a potential cohort study. Fiaccadori E, Maggiore U, Giacosa R, et al: Enteral diet in patients with acute renal failure. Fiaccadori E, Maggiore U, Clima B, et al: Incidence, risk factors, and prognosis of gastrointestinal hemorrhage complicating acute renal failure. Silvester W, Bellomo R, Cole L: Epidemiology, management, and consequence of severe acute renal failure of important illness in Australia. Miltenyi M, Tulassay T, Korner A, et al: Tubular dysfunction in metabolic acidosis: first step to acute renal failure. Pietrek J, Kokot F, Kuska J: Serum 25-hydroxyvitamin D and parathyroid hormone in sufferers with acute renal failure. Zaman F, Abreo K: Severe hypermagnesemia as a end result of laxative use in renal insufficiency. Alderson P, Schierhout G, Roberts I, et al: Colloids versus crystalloids for fluid resuscitation in critically unwell sufferers. Schierhout G, Roberts I: Fluid resuscitation with colloid or crystalloid options in critically ill sufferers: a scientific evaluate of randomised trials. Finfer S, Bellomo R, Boyce N, et al: A comparison of albumin and saline for fluid resuscitation within the intensive care unit. Moreau R, Lebrec D: Diagnosis and treatment of acute renal failure in sufferers with cirrhosis. Ruiz-del-Arbol L, Monescillo A, Arocena C, et al: Circulatory function and hepatorenal syndrome in cirrhosis. Gines P, Tito L, Arroyo V, et al: Randomized comparative research of therapeutic paracentesis with and with out intravenous albumin in cirrhosis. Gines A, Fernandez-Esparrach G, Monescillo A, et al: Randomized trial evaluating albumin, dextran 70, and polygeline in cirrhotic sufferers with ascites handled by paracentesis. Sort P, Navasa M, Arroyo V, et al: Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. Rossle M, Ochs A, Gulberg V, et al: A comparability of paracentesis and transjugular intrahepatic portosystemic shunting in sufferers with ascites. Gines P, Uriz J, Calahorra B, et al: Transjugular intrahepatic portosystemic shunting versus paracentesis plus albumin for refractory ascites in cirrhosis. Salerno F, Camma C, Enea M, et al: Transjugular intrahepatic portosystemic shunt for refractory ascites: a meta-analysis of individual affected person data. Gines P, Torre A, Terra C, et al: Review article: pharmacological remedy of hepatorenal syndrome. Duvoux C, Zanditenas D, Hezode C, et al: Effects of noradrenalin and albumin in sufferers with kind I hepatorenal syndrome: a pilot study. Maioli M, Toso A, Leoncini M, et al: Sodium bicarbonate versus saline for the prevention of contrast-induced nephropathy in sufferers with renal dysfunction undergoing coronary angiography or intervention. Angeli P, Volpin R, Gerunda G, et al: Reversal of type 1 hepatorenal syndrome with the administration of midodrine and octreotide. Moreau R, Durand F, Poynard T, et al: Terlipressin in patients with cirrhosis and kind 1 hepatorenal syndrome: a retrospective multicenter research. Alderson P, Bunn F, Lefebvre C, et al: Human albumin solution for resuscitation and quantity expansion in critically sick patients. Rivers E, Nguyen B, Havstad S, et al: Early goal-directed remedy in the remedy of severe sepsis and septic shock. Budhiraja P, Chen Z, Popovtzer M: Sodium bicarbonate versus normal saline for protection against distinction nephropathy. Zoungas S, Ninomiya T, Huxley R, et al: Systematic evaluation: sodium bicarbonate treatment regimens for the prevention of contrastinduced nephropathy. DiMari J, Megyesi J, Udvarhelyi N, et al: N-acetyl cysteine ameliorates ischemic renal failure. Tepel M, van der Giet M, Schwarzfeld C, et al: Prevention of radiographic-contrast-agent�induced reductions in renal perform by acetylcysteine. Carbonell N, Blasco M, Sanjuan R, et al: Intravenous N-acetylcysteine for preventing contrast-induced nephropathy: a randomised trial. Marenzi G, Assanelli E, Marana I, et al: N-acetylcysteine and contrast-induced nephropathy in major angioplasty. Trivedi H, Daram S, Szabo A, et al: High-dose N-acetylcysteine for the prevention of contrast-induced nephropathy. Cacoub P, Deray G, Baumelou A, et al: No proof for protective results of nifedipine in opposition to radiocontrast-induced acute renal failure.
Kemadrin 5mg low priceDewitte A symptoms ketosis discount kemadrin 5 mg with mastercard, Biais M, Petit L, et al: Fractional excretion of urea as a diagnostic index in acute kidney injury in intensive care sufferers. Cotter G, Metra M, Milo-Cotter O, et al: Fluid overload in acute heart failure-re-distribution and different mechanisms past fluid accumulation. Fauchald P: Colloid osmotic pressures, plasma volume and interstitial fluid volume in sufferers with heart failure. Galanth C, Hus-Citharel A, Li B, et al: Apelin within the control of body fluid homeostasis and cardiovascular functions. Hus-Citharel A, Bouby N, Frugiere A, et al: Effect of apelin on glomerular hemodynamic operate within the rat kidney. Firsov D, Tokonami N, Bonny O: Role of the renal circadian timing system in sustaining water and electrolytes homeostasis. Nikolaeva S, Pradervand S, Centeno G, et al: the circadian clock modulates renal sodium handling. Xiao L, Gao L, Lazartigues E, et al: Brain-selective overexpression of angiotensin-converting enzyme 2 attenuates sympathetic nerve exercise and enhances baroreflex perform in chronic heart failure. Carubelli V, Metra M, Lombardi C, et al: Renal dysfunction in acute heart failure: epidemiology, mechanisms and evaluation. Pagliaro P, Penna C: Rethinking the renin-angiotensin system and its function in cardiovascular regulation. Bohlender J, Imboden H: Angiotensinergic neurotransmission within the peripheral autonomic nervous system. Grassi G, Seravalle G, Quarti-Trevano F, et al: Sympathetic activation in congestive coronary heart failure: evidence, consequences and therapeutic implications. Albaghdadi M, Gheorghiade M, Pitt B: Mineralocorticoid receptor antagonism: therapeutic potential in acute coronary heart failure syndromes. Kaye D, Esler M: Sympathetic neuronal regulation of the guts in getting older and coronary heart failure. Gegenhuber A, Struck J, Dieplinger B, et al: Comparative evaluation of B-type natriuretic peptide, mid-regional pro-A-type natriuretic peptide, mid-regional pro-adrenomedullin, and Copeptin to predict 1-year mortality in sufferers with acute destabilized coronary heart failure. Knecht M, Pagel I, Langenickel T, et al: Increased expression of renal neutral endopeptidase in severe coronary heart failure. Ertl G, Bauersachs J: Endothelin receptor antagonists in coronary heart failure: present standing and future instructions. Ghosh N, Haddad H: Atrial natriuretic peptides in coronary heart failure: pathophysiological significance, diagnostic and prognostic value.
[newline]Liu C, Chen Y, Kang Y, et al: Glucocorticoids improve renal responsiveness to atrial natriuretic peptide by up-regulating natriuretic peptide receptor-A expression within the renal inner medullary accumulating duct in decompensated heart failure. Kobayashi D, Yamaguchi N, Takahashi O, et al: Human atrial natriuretic peptide treatment for acute coronary heart failure: a systematic review of efficacy and mortality. Rubattu S, Calvieri C, Pagliaro B, et al: Atrial natriuretic peptide and regulation of vascular function in hypertension and coronary heart failure: implications for novel therapeutic methods. Krupicka J, Janota T, Kasalova Z, et al: Natriuretic peptides- physiology, pathophysiology and scientific use in heart failure. Longhini C, Molino C, Fabbian F: Cardiorenal syndrome: still not an outlined entity. Castellani S, Paladini B, Paniccia R, et al: Increased renal formation of thromboxane A2 and prostaglandin F2 alpha in heart failure. Kose F, Besen A, Paydas S, et al: Effects of selective Cox-2 inhibitor, rofecoxib, alone or combination with furosemide on renal features and renal Cox-2 expression in rats. Harirforoosh S, Jamali F: Renal antagonistic effects of nonsteroidal anti-inflammatory drugs. Nishikimi T, Matsuoka H: Cardiac adrenomedullin: its function in cardiac hypertrophy and coronary heart failure. Adlbrecht C, Hulsmann M, Strunk G, et al: Prognostic value of plasma midregional pro-adrenomedullin and C-terminalpro-endothelin-1 in persistent heart failure outpatients. Potocki M, Ziller R, Mueller C: Mid-regional pro-adrenomedullin in acute coronary heart failure: a better biomarker or just another biomarker Cinar O, Cevik E, Acar A, et al: Evaluation of mid-regional proatrial natriuretic peptide, procalcitonin, and mid-regional pro- 459. Hirose T, Totsune K, Mori N, et al: Increased expression of adrenomedullin 2/intermedin in rat hearts with congestive heart failure. Liu L, Ding W, Li R, et al: Plasma levels and diagnostic value of catestatin in patients with heart failure. Beltowski J, Rachanczyk J, Wlodarczyk M: Thiazolidinedioneinduced fluid retention: current insights into the molecular mechanisms. Van de Casteele M, Omasta A, Janssens S, et al: In vivo gene switch of endothelial nitric oxide synthase decreases portal pressure in anaesthetised carbon tetrachloride cirrhotic rats. Martell M, Coll M, Ezkurdia N, et al: Physiopathology of splanchnic vasodilation in portal hypertension. Leiper J, Nandi M, Torondel B, et al: Disruption of methylarginine metabolism impairs vascular homeostasis. Bernardi M, Trevisani F, Gasbarrini A, et al: Hepatorenal issues: position of the renin-angiotensin-aldosterone system. Lopez C, Jimenez W, Arroyo V, et al: Temporal relationship between the decrease in arterial strain and sodium retention in aware spontaneously hypertensive rats with carbon tetrachloride-induced cirrhosis. Wong F, Sniderman K, Blendis L: the renal sympathetic and renin-angiotensin response to lower physique unfavorable pressure in well-compensated cirrhosis. Wong F, Liu P, Blendis L: the mechanism of improved sodium homeostasis of low-dose losartan in preascitic cirrhosis. Iwakiri Y: Endothelial dysfunction within the regulation of cirrhosis and portal hypertension. Levy M: Pathogenesis of sodium retention in early cirrhosis of the liver: evidence for vascular overfilling. Bellot P, Frances R, Such J: Pathological bacterial translocation in cirrhosis: pathophysiology, prognosis and scientific implications. Fagundes C, Gines P: Hepatorenal syndrome: a extreme, but treatable, explanation for kidney failure in cirrhosis. Bomzon A, Rosenberg M, Gali D, et al: Systemic hypotension and decreased pressor response in canines with chronic bile duct ligation. Ryan J, Sudhir K, Jennings G, et al: Impaired reactivity of the peripheral vasculature to pressor agents in alcoholic cirrhosis. Wong F, Logan A, Blendis L: Hyperinsulinemia in preascitic cirrhosis: results on systemic and renal hemodynamics, sodium homeostasis, forearm blood flow, and sympathetic nervous exercise. Unifying speculation of body fluid quantity regulation: implications for cardiac failure and cirrhosis. Claria J, Jimenez W, Arroyo V, et al: Effect of V1-vasopressin receptor blockade on arterial stress in conscious rats with cirrhosis and ascites. Arroyo V, Claria J, Salo J, et al: Antidiuretic hormone and the pathogenesis of water retention in cirrhosis with ascites. Tsiakalos A, Hatzis G, Moyssakis I, et al: Portopulmonary hypertension and serum endothelin ranges in hospitalized sufferers with cirrhosis.
References - Lucioni, A., Rapp, D.E., Gong, E.M., Fedunok, P., Bales, G.T. Intravesical botulinum type A toxin injection in patients with overactive bladder: Trigone versus trigonesparing injection. Can J Urol 2006;13:3291-3295.
- Ziaee, S.A., Halimiasl, P., Aminsharifi, A. et al. Management of 10-15-mm proximal ureteral stones: ureteroscopy or extracorporeal shockwave lithotripsy? Urology 2008;71: 28-31.
- Comparison of sustained-release nifedipine and temperature biofeedback for treatment of primary Raynaud phenomenon. Results from a randomized clinical trial with 1-year follow-up, Arch Intern Med 160:1101-1108, 2000.
- Lecci A, Maggi CA: Tachykinins as modulators of the micturition reflex in the central and peripheral nervous system, Regul Pept 101(1n3):1n18, 2001.
- Turner B, Harold E, Matloff E, et al. BRCA1/BRCA2 germline mutations in locally recurrent breast cancer patients after lumpectomy and radiation therapy: implications for breast-conserving management in patients with BRCA1/BRCA2 mutations. J Clin Oncol 1999;17(10):3017-3024.
- Suh JH, Shin OR, Kim YH. Multiple calcifying fibrous pseudotumor of the pleura. J Thorac Oncol 2008;3(11): 1356-8.
|